
 | ||
Gluten-related disorders is the umbrella term for all diseases triggered by gluten. Gluten-related disorders include celiac disease (CD), non-celiac gluten sensitivity (NCGS), gluten ataxia, dermatitis herpetiformis (DH) and wheat allergy. "Gluten intolerance" and "gluten sensitivity" are sometimes used as synonyms for gluten-related disorders, though a multi-disciplinary physician-led study, based in part on the 2011 International Coeliac Disease Symposium, concluded that the use of these terms should be avoided due to a lack of specificity.
Contents
- Types
- Autoimmune disorders
- Coeliac disease
- Dermatitis herpetiformis
- Non celiac gluten sensitivity NCGS
- Wheat allergy
- Other conditions
- Symptoms
- Causes
- Immunochemistry of glutens
- Pathophysiology
- Genetics
- Complications
- Diagnosis
- Treatment
- Epidemiology
- Regulations
- References
Gluten, named from the Latin gluten meaning glue, is a substance that gives elasticity to dough helping it to rise and to keep its shape. It is found in many staple foods in the Western diet.
Currently, there is a growing incidence of a wide spectrum of gluten-related disorders all around the world, including CD and NCGS, as well as gluten-sensitive enteropathy–associated conditions. The increase may be explained by the progressive westernization of diet, the expanded reach of the Mediterranean diet (which includes a lot of foods that incorporate gluten), the growing replacement of rice by wheat in many countries, the development in recent years of new types of wheat with a higher amount of cytotoxic gluten peptides, and the higher content of gluten in bread and bakery products, due to the reduction of dough fermentation time.
Types
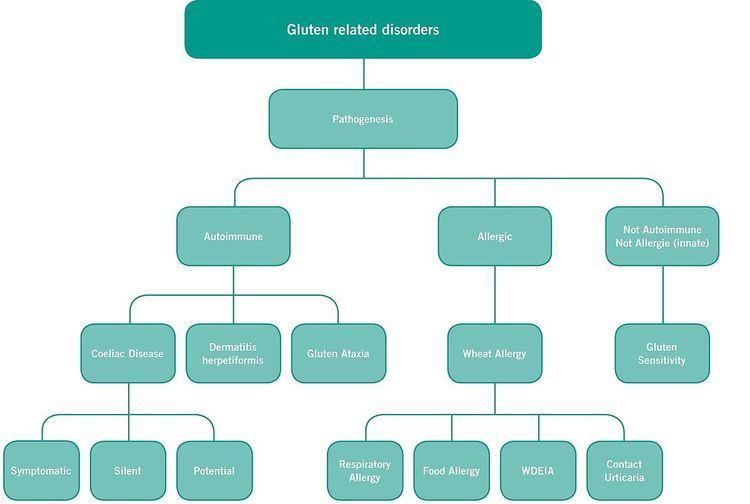
The following classification of gluten-related disorders was announced 2011 by an expert's panel in London, published 2012 and further expanded on later that year:
Autoimmune disorders
Autoimmune conditions related to gluten include celiac disease, dermatitis herpetiformis, and gluten ataxia. There is research showing that in certain patients with gluten ataxia early diagnosis and treatment with a gluten-free diet can improve ataxia and prevent its progression. The population of patients with gluten ataxia and other neurological conditions appears to have a different HLA distribution, in particular more HLA-DQ1, compared to the population of typical celiac disease patients who have HLA-DQ2 and HLA-DQ8.
Coeliac disease
Coeliac disease (American English: celiac) (CD) is one of the most common chronic, immune-mediated disorders, triggered by the eating of gluten, a mixture of proteins found in wheat, barley, rye and derivatives. Evidence has shown that this condition not only has an environmental component but a genetic one as well, due to strong associations of CD with the presence of HLA (Human leukocyte antigen) type II, specifically DQ2 and DQ8 alleles. These alleles can stimulate a T cell, mediated immune response against tissue transglutaminase (TTG), an enzyme in the extracellular matrix, leading to inflammation of the intestinal mucosa and eventually villous atrophy of the small intestine. This is where the innate and adaptive immune response systems collide.
CD is not only a gastrointestinal disease, because it may involve to several organs and cause an extensive variety of non-gastrointestinal symptoms, and most importantly, it may often be completely asymptomatic. Added difficulties for diagnosis are the fact that serological markers (anti-tissue transglutaminase [TG2]) are not always present and many patients may have minor mucosal lesions, without atrophy of the intestinal villi. Diagnosis of CD should be based on a combination of patient’s familial history, genetics (i.e. presence of HLA DQ2/DQ8) serology and intestinal histology.
CD affects approximately 1–2% of general population all over the world, but most cases remain unrecognized, undiagnosed and untreated, and exposed to the risk of long-term complications. Patients may suffer severe disease symptoms and be subjected to extensive investigations for many years, before a proper diagnosis is achieved. Untreated CD may result in the lack of absorption of nutrients, reduced quality of life, iron deficiency, osteoporosis, an increased risk of intestinal lymphomas and greater mortality. CD is associated with some autoimmune diseases, such as diabetes mellitus type 1, thyroiditis, gluten ataxia, psoriasis, vitiligo, autoimmune hepatitis, dermatitis herpetiformis, primary sclerosing cholangitis, and more.
CD with “classic symptoms”, which include gastrointestinal manifestations such as chronic diarrhea and bloating, malabsorption of certain vitamins and minerals, lose of appetite, impaired growth and even bone pain, is currently the least common presentation form of the disease and affects predominantly to small children generally younger than two years of age.
CD with “non-classic symptoms” is the most common clinical found type and occurs in older children (over 2 years old), adolescents and adults. It is characterized by milder or even absent gastrointestinal symptoms and a wide spectrum of non-intestinal manifestations that can involve any organ of the body such as, cerebellar ataxia, hypertransaminasemia and peripheral neuropathy. As previously mentioned, CD although very frequently may be completely asymptomatic both in children (at least in 43% of the cases) and adults.
To date, the only available medically accepted treatment for people with coeliac disease is to follow a lifelong gluten-free diet.
Dermatitis herpetiformis
Dermatitis herpetiformis (DH), or Duhring-Brocq disease, is a chronic blistering skin autoimmune condition, characterized by the presence of skin lesions that have an extensive and symmetrical distribution, predominating in areas of greater friction, and affecting mainly both elbows, knees, buttocks, ankles, and may also affect the scalp and other parts of the body, and non-symmetrical occasionally. The lesions are vesicular-crusted and when flake off, they evolve to pigmented areas or achromic an intense burning, itchy and blistering rash. Despite its name, DH is neither related to nor caused by herpes virus: the name means that it is a skin inflammation having an appearance similar to herpes.
The age of onset is variable starting in children and adolescence but can also affect individuals of both sexes indistinctly at any age of their lives.
A fact that difficults its diagnosis is the relatively common presentation with atypical manifestations. Some patients may show erythema or severe pruritus alone, wheals of chronic urticaria, purpuric lesions resembling petechiae on hands and feet, palmo-plantar keratosis, leukocytoclastic vasculitis-like appearance, and/or lesions mimicking prurigo pigmentosa. DH may be confused with many different cutaneous lesions, such as atopic dermatitis, eczema, urticaria, scabies, impetigo, polymorphic erythema and other autoimmune blistering diseases.
DH is considered to be as "the coeliac disease of the skin". For this reason, the new guidelines of the European Society for Pediatric Gastroenterology, Hepatology and Nutrition for the diagnosis of coeliac disease conclude that its proven presence, by itself, confirms the diagnosis of coeliac disease. Nevertheless, duodenal biopsy is recommended in doubtful DH cases, or if there are suspected gastrointestinal complications, including lymphoma. People with DH have different degrees of intestinal involvement, ranging from milder mucosal lesions to the presence of villous atrophy.
The main and more efficacious treatment for DH is following a lifelong gluten-free diet, which produces the improvement of skin and gut lesions. Nevertheless, the skin lesions may take several months or even years to disappear. To calm itching, dapsone is often recommended as a temporary treatment, during the time it takes for the diet to work, but it has no effect on the gastrointestinal changes and may have important side effects.
Non-celiac gluten sensitivity (NCGS)
Non-celiac gluten sensitivity (NCGS), or gluten sensitivity (GS), is a syndrome in which patients develop a variety of intestinal and/or extraintestinal symptoms that improve when gluten is removed from the diet, after coeliac disease and wheat allergy are excluded. NCGS, which is possibly immune-mediated, now appears to be more common than coeliac disease, with a prevalence estimated to be 6–10 times higher.
Gastrointestinal symptoms, which resemble those of irritable bowel syndrome (IBS), may include any of the following: abdominal pain, bloating, bowel habit abnormalities (either diarrhea or constipation), nausea, aerophagia, gastroesophageal reflux disease, and aphthous stomatitis.
Extra-intestinal symptoms, which can be the only manifestation of NCGS even in absence of gastrointestinal symptoms, may be any of the following: headache or migraine, “foggy mind”, fatigue, fibromyalgia, joint and muscle pain, leg or arm numbness, tingling of the extremities, dermatitis (eczema or skin rash), atopic disorders, allergy to one or more inhalants, foods or metals (such as mites, graminaceae, parietaria, cat or dog hair, shellfish, or nickel), depression, anxiety, anemia, iron-deficiency anemia, folate deficiency, asthma, rhinitis, eating disorders, or autoimmune diseases.
Among extra-intestinal manifestations, NCGS seems to be involved in some neuropsychiatric disorders, principally schizophrenia, autism and peripheral neuropathy, and also ataxia and attention deficit hyperactivity disorder (ADHD).
Gluten is likely responsible for the appearance of symptoms, but it has been suggested than in a subgroup of patients with NCGS and symptoms like IBS, other components of wheat and related grains (oligosaccharides like fructans), or other plant proteins contained in glutencontaining cereals (agglutinins, lectins, and ATIs) may play a role in the development of gastrointestinal symptoms. ATIs are about 2–4% of the total protein in modern wheat and 80–90% in gluten. In a review of May 2015 published in Gastroenterology, Fasano et al. conclude that ATIs may be the inducers of innate immunity in people with coeliac disease or NCGS, and FODMAPs that are present in glutencontaining grains cause mild wheat intolerance at most, which is mainly limited to gastrointestinal symptoms.
As occurs in patients with coeliac disease, the treatment is a gluten-free diet (GFD) strict and maintained, without making any dietary transgression. Whereas coeliac disease requires adherence to a strict lifelong gluten-free diet, it is not yet known whether NCGS is a permanent, or a transient condition. Theoretically, a trial of gluten reintroduction to observe reaction after 1–2 years of strict gluten-free diet might be advisable.
Approximately one third of NCGS patients continue having symptoms despite gluten withdrawal. This may be due to diagnostic error, poor dietary compliance, or other reasons. Those afflicted with NCGS may be under the impression that they don't need to follow a strictly gluten free diet. However, the ingestion of even a small amount of gluten may cause more immediate symptoms in people suffering from NCGS as compared with those afflicted with coeliac disease. People with NCGS should carefully read ingredient labels on food and be aware of potential cross contamination as a source of gluten in otherwise gluten-free foods. To find out if there are unintended ingestions of gluten, an exhaustive evaluation with the advice of a coeliac disease specialized dietitian could be necessary.
In some cases, patients can significantly improve with a low FODMAPs diet in addition to gluten withdrawal and/or a GFD with a low content of preservatives and additives. Furthermore, associated to gluten sensitivity, NCGS people may often present IgE-mediated allergies to one or more foods and it is estimated that around 35% of patients suffer some food intolerances, mainly lactose intolerance.
Wheat allergy
People can also experience adverse effects of wheat as result of a wheat allergy. Gastrointestinal symptoms of wheat allergy are similar to those of coeliac disease and non-celiac gluten sensitivity, but there is a different interval between exposure to wheat and onset of symptoms. Wheat allergy has a fast onset (from minutes to hours) after the consumption of food containing wheat and could be anaphylaxis.
The treatment of wheat allergy consists of complete withdrawal of any food containing wheat and other gluten-containing cereals. Nevertheless, some patients can tolerate barley, rye or oats.
Other conditions
Antibodies to α-gliadin have been significantly increased in non-celiacs individuals with oral ulceration. Anti-α-gliadin antibodies are frequently found in celiac disease (CD), to a lesser degree subclinical CD, but are also found in a subset who do not have the disease. Of people with pseudo-exfoliation syndrome, 25% showed increased levels of anti-gliadin IgA. One fourth of people with Sjögren's syndrome had responses to gluten, of 5 that had positive response to gluten, only one could be confirmed as CD and another was potentially GSE, the remaining 3 appear to be gluten-sensitive. All were HLA-DQ2 and/or DQ8-positive.
Symptoms
More than 250 symptoms of gluten sensitivity have been reported, including bloating, abdominal discomfort or pain, constipation and diarrhea. Sensitivity may also present with extraintestinal symptoms, including headache, "brain fog", tingling and/or numbness in hands and feet, fatigue, as well as muscular disturbances and bone or joint pain; also neuropsychiatric manifestations ("gluten-sensitive idiopathic neuropathies") have been reported on.
Causes
When enteropathy develops in early childhood, symptomatic disease is more rapidly evident. A survey of geriatrics with celiac disease in Finland revealed that the incidence of disease was much higher than the general population. Allergic disease may rise or fall with age; certain evidence points to the increased or daily use of non-steroidal anti-inflammatory factors (aspirin, ibuprofen) as an increased risk factor for urticaria or anaphylaxis, and the sensitizing dose may include low-dose aspirin therapy used in the treatment of heart disease. NCGS may be a late-onset condition: in a prospective study performed among adults of 18 to 80 years, the median age of disease onset was found to be 55 years, with a six times higher prevalence in females than in males.
In a recent double-blind, placebo-controlled challenge (DBPC) by Biesiekierski et al. in a few patients with IBS, the authors found no difference between gluten or placebo groups and the concept of NCGS as a syndrome was questioned. Nevertheless, probably the reintroduction of both gluten and whey protein had a nocebo effect similar in all patients, and this could have masked the true effect of gluten/wheat reintroduction.
Immunochemistry of glutens
Triticeae glutens are important factors in several inflammatory diseases. The immunochemistry can be subdivided into innate responses (direct stimulation of immune system), class II mediated presentation (HLA-DQ), class I mediated stimulation of killer cells, and antibody recognition. The responses to gluten proteins and polypeptide regions differs according to the type of gluten sensitivity. The response is also dependent on the genetic makeup of the human leukocyte antigen genes. In enteropathy, there are at least 3 types of recognition, innate immunity (a form of cellular immunity priming), HLA-DQ and antibody recognition of gliadin and transglutaminase. In NCGS, there is high AGA IgG in more than half of the cases. In wheat allergy, there appears to be an innate component and the response pathways are mediated through IgE against gliadin and other wheat proteins.
Pathophysiology
Compared to the pathophysiology of celiac disease, the pathophysiology of NCGS is far less understood.
A literature review of 2014 found that patients suffering from NCGS "are a heterogeneous group, composed of several subgroups, each characterized by different pathogenesis and clinical history, and, probably, clinical course".
Genetics
Celiac disease (CD) and NCGS are closely linked with human leukocyte antigen (HLA) class II genes, HLA-DQ2 and HLA-DQ8, located on chromosome 6p21. Nearly all CD patients are NLA-DQ2/HLA-DQ8 positive, with 95% HLA-DQ2 and the rest usually HLA-DQ8 (which is carried by 30% of Caucasians). However, the specificity of HLA-DQ2 and/or HLA-DQ8 for CD is low, with estimates ranging from 36% to 53%. In NCGS patients, the HLA-DQ2 and/or HLA-DQ8 alleles are present in only about 50%, which is still a greater proportion than in the general population.
Complications
Studies using anti-gliadin antibodies (AGA) reveal that diagnosed or untreated individuals with AGA have an increasing risk for lymphoid cancers and decreased risk for other conditions associated with affluence.
Diagnosis
A literature review of 2014 found that non-coeliac gluten sensitivity diagnosis can be reached only by excluding celiac disease (CD) and wheat allergy.
Persons suspected of having celiac disease may undergo serological testing for IgA anti-tissue transglutaminase antibodies (abbreviated anti-tTG antibodies or anti-TG2 antibodies) and anti-endomysial antibodies (abbreviated EMA) provided the IgA-level is high, and if IgA is low, testing for certain IgG antibodies; in case of positive serological indication, a duodenal biopsy may confirm active celiac disease.
Eliminating the possibility of CD can generally also be done by adding HLA-DQ typing. The absence of HLA-DQ2 and HLA-DQ8 has a very high negative predictive value for CD, and the predictive value can be further enhanced by including HLA-DQ7.5 (HLA-DQ2 and HLA-DQ8 are found in coeliac disease 98% of the time in Caucasians, HLA-DQ7.5 present in the remaining 1.6% and only 0.4% of Caucasians are missed with the combination of these 3). Without serological or HLA-DQ2/8 positivity, celiac disease is likely not present. HLA-DQ typing has a practical advantage in that it is the only diagnostic test that allows to exclude CD when a patient is already on a gluten-free diet; however, as not only celiacs are HLA-DQ2/HLA-DQ8 positive, this method has a higher false positive rate than anti-TG2 and EMA antibody testing.
A four-of-five rule was proposed 2010 for confirming celiac disease, with the disease confirmed if at least four of the following five criteria are satisfied:
For diagnosis of wheat allergy, allergy tests are available.
Treatment
For patients with celiac disease, a lifelong strict gluten-free diet is the only effective treatment to date; for patients diagnosed with NCGS, there are still open questions concerning for example the duration of such a diet; for patients with wheat allergy, the individual average is six years of gluten-free diet, excepting persons with anaphylaxis, for whom the diet is to be wheat-free for life.
A gluten-free diet should not be started before the tests for excluding celiac disease have been performed, for the reason that the serological and biopsy tests for celiac disease are reliable only if the patient is consuming gluten.
Preferably, newly diagnosed celiacs seek the help of a dietician to receive support for identifying hidden sources of gluten, planning balanced meals, reading labels, food shopping, dining out, and dining during travel. Knowledge of hidden sources of gluten is important for celiac disease patients as they need to be very strict regarding eating only gluten-free food; for NCGS patients, it is not certain how strict the diet needs to be. Balanced eating is important because unless particular care is taken, a gluten-free diet can be lacking in vitamins, minerals, and fiber, and be too high in fat and calories.
The inclusion of oats in gluten-free diets remains controversial. Avenin present in oats may also be toxic for coeliac sufferers. Its toxicity depends on the cultivar consumed. Furthermore, oats are frequently cross-contaminated with gluten-containing cereals.
Epidemiology
The incidence of celiac disease and of wheat allergy is estimated each to lie at around 1% of the population. The incidence of NCGS is unknown; some estimates range from 0.6% to 6%, and a systematic review of 2015 reported on studies with NCGS prevalence rates between 0.5% and 13%.
In Europe, the average consumption of gluten is 10g to 20g per day, with parts of the population reaching 50g or more per day.
Regulations
In various countries, regulations and labelling requirements for gluten-free food products have been implemented.
For Europe, the Commission Regulation (EC) No. 41/2009 of 20 January 2009 concerning the composition and labelling of foodstuffs suitable for people intolerant to gluten has laid down harmonised rules on the content and labelling of these foodstuffs, setting out the conditions under which foods may be labelled as "gluten-free" or "very low gluten". Having entered into force on 10 February 2009 and taken effect on 1 January 2012, these rules have been repealed with effect as of 20 July 2016. The background is that, in line with the Regulation (EU) No 609/2013 on food for specific groups, gluten-free foods shall, in future, be legislated for under the EU Food Information for Consumers Regulation (Regulation (EU) No. 1169/2011). Furthermore, the Commission Implementing Regulation (EU) No 828/2014 of 30 July 2014 on the requirements for the provision of information to consumers on the absence or reduced presence of gluten in food extends the rules of Regulation (EC) 41/2009 on "gluten-free" and "very low gluten" statements also to non pre-packed foods such as those served in restaurants. The implementing regulation also clarifies how consumers are to be informed of the difference between foods that are naturally free of gluten and products that are specially formulated for gluten-intolerant persons.
Recognition of gluten-free packaged foods is facilitated by the crossed-grain symbol, representing a crossed ear of wheat. The symbol is used as a logo that facilitates food shopping for patients with CD and other gluten-related disorders. The symbol, which is protected as a trademark in Europe and the United States and is covered by worldwide copyright, can be represented in any colour.