
OMIM 103900 | ICD-9-CM 255.11 | |
 | ||
Glucocorticoid remediable aldosteronism (GRA), also describable as aldosterone synthase hyperactivity, is an autosomal dominant disorder in which the increase in aldosterone secretion produced by ACTH is no longer transient.
Contents
It is a cause of primary hyperaldosteronism.
Symptoms
Patients with GRA may be asymptomatic, but the following symptoms can be present:
Normal Physiology
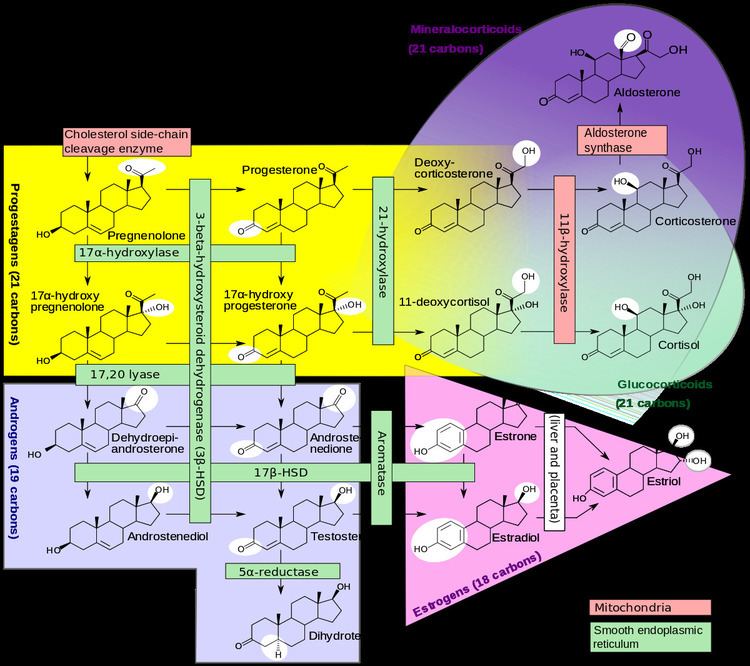
Aldosterone synthase is a steroid hydroxylase cytochrome P450 oxidase enzyme involved in the generation of aldosterone. It is localized to the mitochondrial inner membrane. The enzyme has steroid 18-hydroxylase activity to synthesize aldosterone and other steroids. Aldosterone synthase is found within the zona glomerulosa at the outer edge of the adrenal cortex. Aldosterone synthase normally is not ACTH sensitive, and only activated by angiotensin II.
Aldosterone causes the tubules of the kidneys to retain sodium and water. This increases the volume of fluid in the body, and drives up blood pressure.
Steroid hormones are synthesized from cholesterol within the adrenal cortex. Aldosterone and corticosterone share the first part of their biosynthetic pathway. The last part is either mediated by the aldosterone synthase (for aldosterone) or by the 11β-hydroxylase (for corticosterone).
Aldosterone synthesis is stimulated by several factors:by increase in the plasma concentration of angiotensin III.by increased plasma angiotensin II, ACTH, or potassium levels.The ACTH stimulation test is sometimes used to stimulate the production of aldosterone along with cortisol to determine if primary or secondary adrenal insufficiency is present.by plasma acidosis.by the stretch receptors located in the atria of the heart.by adrenoglomerulotropin, a lipid factor, obtained from pineal extracts. It selectively stimulates secretion of aldosterone.The secretion of aldosterone has a diurnal rhythm.Control of aldosterone release from the adrenal cortex:Pathophysiology
The genes encoding aldosterone synthase and 11-hydroxylase are 95% identical and are close together on chromosome 8. In individuals with GRA, there is unequal crossing over so that the 5' regulatory region of the 11-hydroxylase gene is fused to the coding region of the aldosterone synthase.
The product of this hybrid gene is aldosterone synthase that is ACTH-sensitive in the zona fasciculata of the adrenal gland.
Although in normal subjects, ACTH accelerates the first step of aldosterone synthesis, ACTH normally has no effect on the activity of aldosterone synthase. However, in subjects with glucocorticoid-remediable aldosteronism, ACTH increases the activity of existing aldosterone synthase, resulting in an abnormally high rate of aldosterone synthesis and hyperaldosteronism.
Treatment
In GRA, the hypersecretion of aldosterone and the accompanying hypertension are remedied when ACTH secretion is suppressed by administering glucocorticoids.
Dexamethasone, spironolactone and eplerenone have been used in treatment.