
Synonyms acute supraglottitis ICD-10 J05.1 DiseasesDB 4360 | Specialty pulmonology ICD-9-CM 464.3, 476.1 MedlinePlus 000605 | |
 | ||
Epiglottitis is inflammation of the epiglottis—the flap at the base of the tongue that keeps food from going into the trachea (windpipe). Symptoms are usually rapid in onset and include trouble swallowing which can result in drooling, changes to the voice, fever, and an increased breathing rate. As the epiglottis is in the upper airway, swelling can interfere with breathing. People may lean forward in an effort to open the airway. As the condition worsens stridor and bluish skin may occur.
Contents
- Signs and symptoms
- Cause
- Diagnosis
- Prevention
- Airway management
- Antibiotics
- Epidemiology
- Complications
- Notable deaths
- References
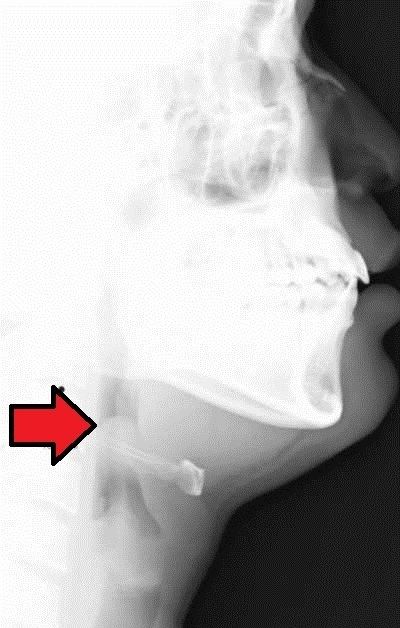
Epiglottitis was historically mostly caused by infection by H. influenzae type b. With vaccination it is now more often caused by other bacteria. Other possible causes include burns and trauma to the area. The most accurate way to make the diagnosis is to look directly at the epiglottis. X-rays of the neck from the side may show a "thumbprint sign" but the lack of this sign does not mean the condition is absent.
An effective vaccine, the Hib vaccine, has been available since the 1980s. The antibiotic rifampin may also be used to prevent the disease among those who have been exposed to the disease and are at high risk. The most important part of treatment involves securing the airway, which is often done by endotracheal intubation. Intravenous antibiotics such as ceftriaxone and possibly vancomycin or clindamycin is then given. Corticosteroids are also typically used. With appropriate treatment, the risk of death among children with the condition is about one percent and among adults is seven percent.
With the use of the Hib vaccine, the number of cases of epiglottitis has decreased by more than 95%. While historically young children were mostly affected, it is now more common among older children and adults. In the United States it affects about 1.3 per 100,000 children a year. In adults between 1 and 4 per 100,000 are affected a year. It occurs more commonly in the developing world. In children the risk of death is about 6%; however, if they are intubated early is less than 1%.
Signs and symptoms
Epiglottitis is associated with fever, difficulty in swallowing, drooling, hoarseness of voice, and typically stridor. Stridor is a sign of upper airways obstruction and is a surgical emergency. The child often appears acutely ill, anxious, and has very quiet shallow breathing with the head held forward, insisting on sitting up in bed. The early symptoms are insidious but rapidly progressive, and swelling of the throat may lead to cyanosis and asphyxiation.
Since the introduction of the Hemophilus influenzae (Hib) vaccination in many Western countries, childhood incidence has decreased while adult incidence has remained the same; the disease is thus becoming relatively more common in adults than children.
Cause
Epiglottitis is typically due to a bacterial infection of the epiglottis. While it historically was most often caused by Haemophilus influenzae type B with immunization this is no longer the case. Bacteria that are now typically involved are Streptococcus pneumoniae, Streptococcus pyogenes, or Staphylococcus aureus.
Other possible causes include burns and trauma to the area. Epiglottitis has been linked to crack cocaine usage. Graft versus host disease and lymphoproliferative disorder can also be a cause.
Diagnosis
Diagnosis is confirmed by direct inspection using laryngoscopy, although this may provoke airway spasm. If epiglottitis is suspected, attempts to visualise the epiglottis using a tongue depressor are strongly discouraged for this reason; therefore, diagnosis is made on basis of direct fibreoptic laryngoscopy carried out in controlled environment like an operating room. Imaging is rarely useful, and treatment should not be delayed for this test to be carried out.
The epiglottis and arytenoids are cherry-red and swollen. The most likely differential diagnostic candidates are croup, peritonsillar abscess, and retropharyngeal abscess.
On lateral C-spine X-ray, the thumbprint sign describes a swollen, enlarged epiglottis; usually with dilated hypopharynx and normal subglottic structures.
On CT imaging, the "halloween sign" describe a normal thickness epiglottis. It can safely exclude the acute epiglottitis. Furthermore, CT imaging can help to diagnose other conditions such as peritonsillar abscess or retropharyngeal abscess which had similar clinical features.
Prevention
The Hib vaccine is very effective at preventing the disease.
In household contacts of any unvaccinated child infected with H. influenzae, rifampicin is used as prophylaxis.
Airway management
Epiglottitis may require urgent tracheal intubation to protect the airway, though this is not always the case. A surgical airway opening (cricothyrotomy) may be required if intubation is not possible.
Antibiotics
In addition, people should be given antibiotics, such as second- or third-generation cephalosporins, either alone or in combination with penicillin or ampicillin for streptococcal coverage. If allergy to penicillins is present, Co-trimoxazole or clindamycin is an alternative.
Epidemiology
While historically young children were mostly affected, it is now more common among older children and adults. Before immunization children of two to four were most commonly affected. With immunization about 1.3 per 100,000 children are affected a year.
Complications
Some patients may develop pneumonia, lymphadenopathy, or septic arthritis.
Notable deaths
George Washington is one historical figure thought to have died of epiglottitis.