
Specialty cardiology ICD-9-CM 423.2 eMedicine article/157096 | ICD-10 I31.1 MedlinePlus 001103 MeSH D010494 | |
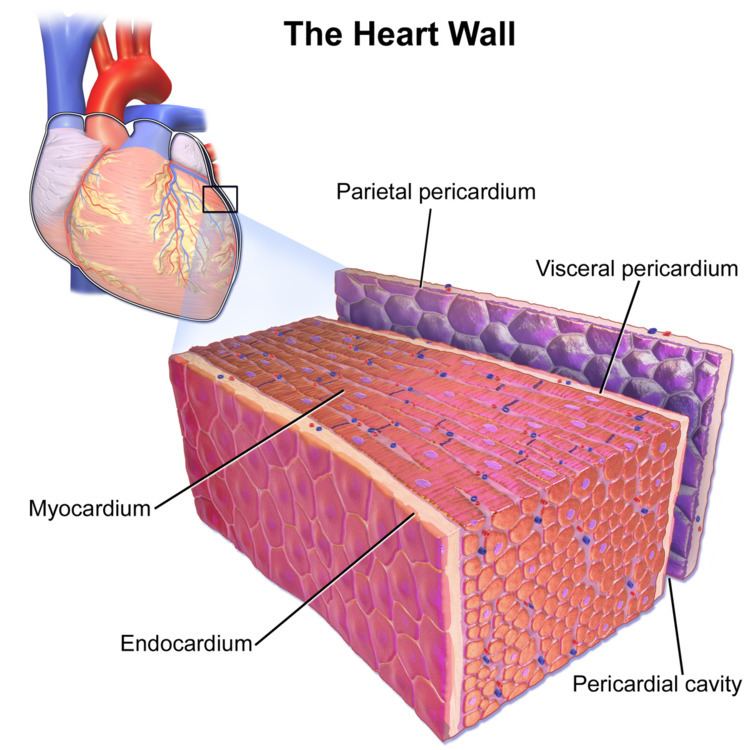 | ||
Constrictive pericarditis is a medical condition characterized by a thickened, fibrotic pericardium, limiting the heart's ability to function normally. In many cases, the condition continues to be difficult to diagnose and therefore benefits from a good understanding of the underlying cause.
Contents
Signs and symptoms
Signs and symptoms of constrictive pericarditis are consistent with the following: fatigue, swollen abdomen, difficulty breathing (dyspnea), swelling of legs and general weakness. Related conditions are bacterial pericarditis, pericarditis and pericarditis after a heart attack.
Causes
The cause of constrictive pericarditis in the developing world are idiopathic in origin, though likely infectious in nature. In regions where tuberculosis is common, it is the cause in a large portion of cases.
Causes of constrictive pericarditis include:
Pathophysiology
The pathophysiological characteristics of constrictive pericarditis are due to a thickened, fibrotic pericardium that forms a non-compliant shell around the heart. This shell prevents the heart from expanding when blood enters it. This results in significant respiratory variation in blood flow in the chambers of the heart.
During inspiration, pressure in the thoracic cavity decreases but is not relayed to the left atrium, subsequently a reduction in flow to the left atrium and ventricle happens. During diastole, less blood flow in left ventricle allows for more room for filling in right ventricle and therefore a septal shift occurs.
During expiration, the amount of blood entering the right ventricle will decrease, allowing the interventricular septum to bulge towards the right ventricle, and increased filling of the left ventricle and subsequent increased pressure generated by the left ventricle during systole.This is known as ventricular interdependence, since the amount of blood flow into one ventricle is dependent on the amount of blood flow into the other ventricle.
Diagnosis
The diagnosis of constrictive pericarditis is often difficult to make. In particular, restrictive cardiomyopathy has many similar clinical features to constrictive pericarditis, and differentiating them in a particular individual is often a diagnostic dilemma.
Treatment
The definitive treatment for constrictive pericarditis is pericardial stripping, which is a surgical procedure where the entire pericardium is peeled away from the heart. This procedure has significant risk involved, with mortality rates of 6% or higher in major referral centers.
A poor outcome is almost always the result after a pericardiectomy is performed for constrictive pericarditis whose origin was radiation-induced,further some patients may develop heart failure post-operatively.