
Latin Canalis carpi TA A03.5.11.201 | Dorlands/Elsevier c_04/12208551 FMA 42352 | |
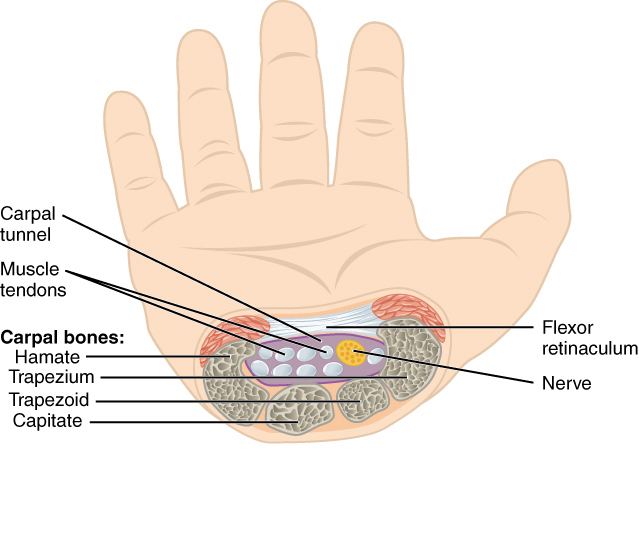 | ||
In the human body, the carpal tunnel or carpal canal is the passageway on the palmar side of the wrist that connects the forearm to the hand.
Contents
The tunnel is bounded by the bones of the wrist and flexor retinaculum from connective tissue. Normally several tendons from the flexor group of forearm muscles and the median nerve pass through it. There are described cases of variable median artery occurrence.
The canal is narrow, and when any of the nine long flexor tendons passing through it swell or degenerate, the narrowing of the canal may result in the median nerve becoming entrapped or compressed, a common medical condition known as carpal tunnel syndrome.
Structure
The carpal bones that make up the wrist form an arch which is convex on the dorsal side of the hand and concave on the palmar side. The groove on the palmar side, the sulcus carpi, is covered by the flexor retinaculum, a sheath of tough connective tissue, thus forming the carpal tunnel. On the side of the radius, the flexor retinaculum is attached to the scaphoid bone, more precisely its tubercle, as well as the ridge of trapezium. On the ulnar side it is attached to the pisiform and hook of hamate.
The narrowest section of the tunnel is located a centimetre beyond the mid-line of the distal row of carpal bones where the sectional area is limited to 1.6 cm2.
The tendons of the flexor digitorum superficialis and profundus pass through a common ulnar sheath, while the tendon of the flexor pollicis longus passes through a separate radial sheath. The mesotendon shared by these tendons is attached to the radial and palmar walls of the carpal tunnel.
Superficial to the carpal tunnel and the flexor retinaculum, the ulnar artery and ulnar nerve pass through the ulnar tunnel.
Function
A total of nine flexor tendons (not the muscles themselves) pass through the carpal tunnel:
A single nerve passes through the tunnel: the median nerve between tendons of flexor digitorum profundus and flexor digitorum superficialis
Effect of wrist movements
Movements in the wrist affect the shape and width of the carpal tunnel. The width decreases considerably during normal range of motion in the wrist and because the carpal bones move in relation to each other with every motion of the hand the bony walls of the tunnel are not rigid. Both flexion and extension increase compression in the carpal tunnel.
Clinical significance
Carpal tunnel syndrome is a syndrome characterised by tingling burning and pain (needle, pin) through the course of median nerve particularly over the outer fingers and radiating up the arm, that is caused by compression of the carpal tunnel contents. It is associated with repetitive use, rheumatoid arthritis, and a number of other states. It can be detected using Tinel's sign and the Phalen maneuver. It may be treated non-surgically by splinting and/or corticosteroid injection, though definitive management often requires surgical division of the flexor retinaculum, which forms the roof of the carpal tunnel.