
Latin Nervus medianus Dorlands/Elsevier n_05/12566162 | MeSH Median+Nerve TA A14.2.03.031 | |
 | ||
Innervates Anterior compartment of the forearm (with two exceptions), Thenar eminence, Lumbricals, skin of the hand | ||
The median nerve is a nerve in humans and other animals in the upper limb. It is one of the five main nerves originating from the brachial plexus.
Contents
The median nerve originates from the lateral and medial cords of the brachial plexus, and has contributions from ventral roots of C5-C7(lateral cord) and C8 & T1 (medial cord).
The median nerve is the only nerve that passes through the carpal tunnel. Carpal tunnel syndrome is the disability that results from the median nerve being pressed in the carpal tunnel.
Structure
After receiving inputs from both the lateral and medial cords of the brachial plexus, the median nerve enters the arm from the axilla at the inferior margin of the teres major muscle. It then passes vertically down and courses with the brachial artery on the medial side of the arm between biceps brachii and brachialis. At first it is lateral to the artery and lies anterior to the elbow joint; it then crosses anteriorly to run medial to the artery in the distal arm and into the cubital fossa.
Inside the cubital fossa the median nerve passes medial to the brachial artery, in front of the point of insertion of the brachialis muscle and deep to the biceps.
The median nerve gives off an articular branch in the upper arm as it passes the elbow joint. A branch to pronator teres may arise from the median nerve immediately proximal to the elbow joint.
Forearm
The median nerve arises from the cubital fossa and passes between the two heads of pronator teres. It then travels between flexor digitorum superficialis and flexor digitorum profundus before emerging between flexor digitorum superficialis and flexor pollicis longus.
The unbranched portion of the median nerve (which arises from the cubital fossa) innervates muscles of superficial and intermediate groups of the anterior(flexor) compartment except flexor carpi ulnaris.
The median nerve does give off two branches as it courses through the forearm:
Hand
The median nerve enters the hand through the carpal tunnel, deep to the flexor retinaculum along with the tendons of flexor digitorum superficialis, flexor digitorum profundus, and flexor pollicis longus.
From there it sends off several branches:
Variation
There are multiple naturally occurring anomalies of the median nerve.
Arm
The median nerve has no voluntary motor or cutaneous function in the brachium. It gives vascular branches to the wall of the brachial artery. These vascular branches carry sympathetic fibers.
Forearm
It innervates all of the flexors in the forearm except flexor carpi ulnaris and that part of flexor digitorum profundus that supplies the 4th and 5th digits. The latter two muscles are supplied by the ulnar nerve (specifically the Muscular branches of ulnar nerve).
The main portion of the median nerve supplies the following muscles:
Superficial group:
Intermediate group:
The anterior interosseus branch of the median nerve supplies the following muscles:
Deep group:
Hand
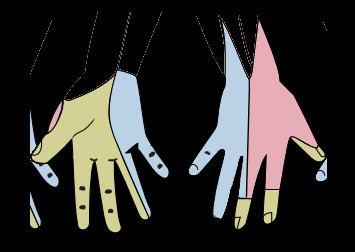
In the hand, the median nerve supplies motor innervation to the 1st and 2nd lumbrical muscles. It also supplies the muscles of the thenar eminence by a recurrent thenar branch. The rest of the intrinsic muscles of the hand are supplied by the ulnar nerve.
The median nerve innervates the skin of the palmar side of the index, the thumb and middle finger, half the ring finger, and the nail bed. The lateral part of the palm is supplied by the palmar cutaneous branch of the median nerve, which leaves the nerve proximal to the wrist creases. This palmar cutaneous branch travels in a separate fascial groove adjacent to the flexor carpi radialis and then superficial to the flexor retinaculum. It is therefore spared in carpal tunnel syndrome.
The muscles of the hand supplied by the median nerve can be remembered using the mnemonic, "LOAF" for Lumbricals 1 & 2, Opponens pollicis, Abductor pollicis brevis and Flexor pollicis brevis. (NB: OAF are the thenar eminence)
Injury
Injury of median nerve at different levels causes different syndromes with varying motor and sensory deficits.
Above the elbow
At the elbow
Within the proximal forearm: Anterior interosseous syndrome
At the wrist
Within the wrist: Carpal tunnel syndrome