
Molar mass 3,020.29 g/mol | Formula C112H179N35O46 | |
 | ||
Insulin c peptide test distinguishing diabetes types
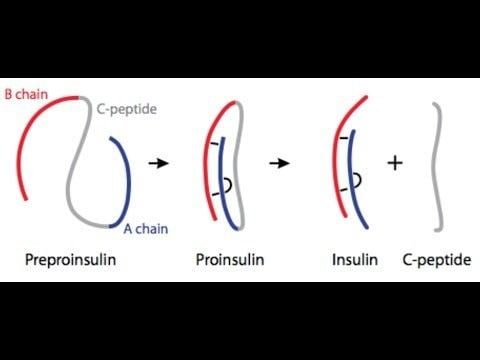
The connecting peptide, or C-peptide, is a short 31-amino-acid polypeptide that connects insulin's A-chain to its B-chain in the proinsulin molecule. In diabetes and other diseases a measurement of C-peptide blood serum levels can be used to distinguish between certain diseases with similar clinical features.
Contents
- Insulin c peptide test distinguishing diabetes types
- C peptide
- History
- Cellular effects of C peptide
- Clinical uses of C peptide testing
- Therapeutics
- References
In the insulin synthesis pathway, first preproinsulin is translocated into the endoplasmic reticulum of beta cells of the pancreas with an A-chain, a C-peptide, a B-chain, and a signal sequence. The signal sequence is cleaved from the N-terminus of the peptide by a signal peptidase, leaving proinsulin. After proinsulin is packaged into vesicles in the Golgi apparatus (beta-granules), the C-peptide is removed, leaving the A-chain B-chain, bound together by disulfide bonds, that constitute the insulin molecule.
C peptide
History
Proinsulin C-peptide was first described in 1967 in connection with the discovery of the insulin biosynthesis pathway. It serves as a linker between the A- and the B- chains of insulin and facilitates the efficient assembly, folding, and processing of insulin in the endoplasmic reticulum. Equimolar amounts of C-peptide and insulin are then stored in secretory granules of the pancreatic beta cells and both are eventually released to the portal circulation. Initially, the sole interest in C-peptide was as a marker of insulin secretion and has, as such, been of great value in furthering the understanding of the pathophysiology of type 1 and type 2 diabetes. The first documented use of the C-peptide test was in 1972. During the past decade, however, C-peptide has been found to be a bioactive peptide in its own right, with effects on microvascular blood flow and tissue health.
Cellular effects of C-peptide
C-peptide has been shown to bind to the surface of a number of cell types such as neuronal, endothelial, fibroblast and renal tubular, at nanomolar concentrations to a receptor that is likely G-protein-coupled. The signal activates Ca2+-dependent intracellular signaling pathways such as MAPK, PLCγ, and PKC, leading to upregulation of a range of transcription factors as well as eNOS and Na+K+ATPase activities. The latter two enzymes are known to have reduced activities in patients with type I diabetes and have been implicated in the development of long-term complications of type I diabetes such as peripheral and autonomic neuropathy.
In vivo studies in animal models of type 1 diabetes have established that C-peptide administration results in significant improvements in nerve and kidney function. Thus, in animals with early signs of diabetes-induced neuropathy, C peptide treatment in replacement dosage results in improved peripheral nerve function, as evidenced by increased nerve conduction velocity, increased nerve Na+,K+ ATPase activity, and significant amelioration of nerve structural changes. Likewise, C-peptide administration in animals that had C-peptide deficiency (type 1 model) with nephropathy improves renal function and structure; it decreases urinary albumin excretion and prevents or decreases diabetes-induced glomerular changes secondary to mesangial matrix expansion. C-peptide also has been reported to have anti-inflammatory effects as well as aid repair of smooth muscle cells. ii
Clinical uses of C-peptide testing
Therapeutics
Therapeutic use of C-peptide has been explored in small clinical trials in diabetic kidney disease. Creative Peptides, Eli Lilly, and Cebix all had drug development programs for a C-peptide product. Cebix had the only ongoing program until it completed a Phase IIb trial in December 2014 that showed no difference between C-peptide and placebo, and it terminated its program and went out of business.