
Specialty pulmonology Duration long term | Usual onset gradual | |
 | ||
Treatment antibiotics, bronchodilators, lung transplant | ||
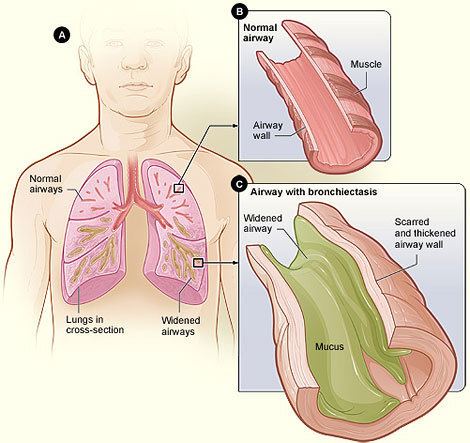
Bronchiectasis is a disease in which there is permanent enlargement of parts of the airways of the lung. Symptoms typically include a chronic cough productive of mucus. Other symptoms include shortness of breath, coughing up blood, and chest pain. Wheezing and nail clubbing may also occur. Those with the disease often get frequent lung infections.
Contents
- Signs and symptoms
- Causes
- Acquired causes
- Congenital causes
- Pathophysiology
- Diagnosis
- Prevention
- Treatment
- Epidemiology
- History
- References
Bronchiectasis may result from a number of infective and acquired causes, including pneumonia, tuberculosis, immune system problems, and cystic fibrosis. Cystic fibrosis eventually results in severe bronchiectasis in nearly all cases. The cause in 10-50% of those without cystic fibrosis is unknown. The mechanism of disease is breakdown of the airways due to an excessive inflammatory response. Involved airways (bronchi) become enlarged and thus less able to clear secretions. These secretions increase the amount of bacteria in the lungs, result in airway blockage and further breakdown of the airways. It is classified as an obstructive lung disease, along with chronic obstructive pulmonary disease and asthma. The diagnosis is suspected based on a person's symptoms and confirmed using computed tomography. Cultures of the mucus produced may be useful to determine treatment in those who have acute worsening and at least once a year.
Worsening may occur due to infection and in these cases antibiotics are recommended. Typical antibiotics used include amoxicillin, erythromycin, or doxycycline. Antibiotics may also be used to prevent worsening of disease. Airway clearance techniques, a type of physical therapy, are recommended. Medications to dilate the airways may be useful in some but the evidence is not very good. The use of inhaled steroids has not been found to be useful. Surgery, while commonly done, has not been well studied. Lung transplantation may be an option in those with very severe disease. While the disease may cause significant health problems most people with the disease do well.
The disease affects between 1 per 1000 to 1 per 250,000 adults. The disease is more common in women and increases as people age. It became less common since the 1950s with the introduction of antibiotics. It is more common among certain ethnic groups such as indigenous people. It was first described by Rene Laennec in 1819. The economic costs in the United States are estimated at $630 million per year.
Signs and symptoms
Some people with bronchiectasis may have a cough productive of frequent green/yellow mucus (sputum) (up to 240ml (8 oz) daily). Bronchiectasis may also present with coughing up blood (hemoptysis) in the absence of sputum, called "dry bronchiectasis". Sputum production may also occur without coloration. People with bronchiectasis may have bad breath indicative of active infection. Frequent bronchial infections and breathlessness are two possible indicators of bronchiectasis.
Crepitations and expiratory rhonchi may be heard on auscultation. Nail clubbing is rare.
Causes
Bronchiectasis has both congenital and acquired causes, with the latter more frequent. Cystic fibrosis is a cause in up to half of cases. The cause in 10-50% of those without cystic fibrosis is unknown; bronchiectasis without CF is known as non-CF bronchiectasis (NCBE).
Acquired causes
Tuberculosis, pneumonia, inhaled foreign bodies, allergic bronchopulmonary aspergillosis and bronchial tumours are the major acquired causes of bronchiectasis. Infective causes associated with bronchiectasis include infections caused by the Staphylococcus, Klebsiella, or Bordetella pertussis, the causative agent of whooping cough.
Aspiration of ammonia and other toxic gases, pulmonary aspiration, alcoholism, heroin (drug use), various allergies all appear to be linked to the development of bronchiectasis.[source needs translation]
Various immunological and lifestyle factors have also been linked to the development of bronchiectasis:
No cause is identified in up to 50% of non-cystic-fibrosis related bronchiectasis.
Congenital causes
Bronchiectasis may result from congenital disorders that affect cilia motility or ion transport. Kartagener syndrome is one such disorder of cilia motility linked to the development of bronchiectasis. A common cause is cystic fibrosis, which affects chloride ion transport, in which a small number of patients develop severe localized bronchiectasis. Young's syndrome, which is clinically similar to cystic fibrosis, is thought to significantly contribute to the development of bronchiectasis. This is due to the occurrence of chronic infections of the sinuses and bronchiole tree.
Other less-common congenital causes include primary immunodeficiencies, due to the weakened or nonexistent immune system response to severe, recurrent infections that commonly affect the lung. Several other congenital disorders can also lead to bronchiectasis, including Williams-Campbell syndrome and Marfan syndrome.
Patients with alpha 1-antitrypsin deficiency have been found to be particularly susceptible to bronchiectasis, for unknown reasons.
Pathophysiology
Bronchiectasis is a result of chronic inflammation compounded by an inability to clear mucoid secretions. This can be a result of genetic conditions resulting in a failure to clear sputum (primary ciliary dyskinesia), or resulting in more viscous sputum (cystic fibrosis), or the result of chronic or severe infections. Inflammation results in progressive destruction of the normal lung architecture, in particular, the elastic fibers of bronchi.
Endobronchial tuberculosis commonly leads to bronchiectasis, either from bronchial stenosis or secondary traction from fibrosis.
Diagnosis
Bronchiectasis may be diagnosed clinically or on review of imaging. The British Thoracic Society recommends all non cystic-fibrosis-related bronchiectasis be confirmed by CT. CT may reveal tree-in-bud abnormalities, dilated bronchi, and cysts with defined borders.
Other investigations typically performed at diagnosis include blood tests, sputum cultures, and sometimes tests for specific genetic disorders.
Prevention
In order to prevent bronchiectasis, children should be immunized against measles, pertussis, pneumonia, and other acute respiratory infections of childhood. While smoking has not been found to be a direct cause of bronchiectasis, it is certainly an irritant that all patients should avoid in order to prevent the development of infections (such as bronchitis) and further complications.
Treatments to slow down the progression of this chronic disease include keeping bronchial airways clear and secretions weakened through various forms of pneumotherapy. Aggressively treating bronchial infections with antibiotics to prevent the destructive cycle of infection, damage to bronchial tubes, and more infection is also standard treatment. Regular vaccination against pneumonia, influenza and pertussis are generally advised. A healthy body mass index and regular doctor visits may have beneficial effects on the prevention of progressing bronchiectasis. The presence of hypoxemia, hypercapnia, dyspnea level and radiographic extent can greatly affect the mortality rate from this disease.
Treatment
Treatment of bronchiectasis includes controlling infections and bronchial secretions, relieving airway obstructions, removal of affected portions of lung by surgical removal or artery embolization and preventing complications. The prolonged use of antibiotics prevents detrimental infections and decreases hospitalizations in people with bronchiectasis. The prolonged use of antibiotics increases the risk of people becoming infected with drug-resistant bacteria.
Other treatment options include eliminating accumulated fluid with postural drainage and chest physiotherapy. Postural drainage techniques, aided by physiotherapists and respiratory therapists, are an important mainstay of treatment. Airway clearance techniques appear useful.
Surgery may also be used to treat localized bronchiectasis, removing obstructions that could cause progression of the disease.
Inhaled steroid therapy that is consistently adhered to can reduce sputum production and decrease airway constriction over a period of time, and help prevent progression of bronchiectasis. This is not recommended for routine use in children. One commonly used therapy is beclometasone dipropionate. Although not approved for use in any country, mannitol dry inhalation powder, has been granted orphan drug status by the FDA for use in people with bronchiectasis and with cystic fibrosis.
Epidemiology
The disease affects between 1 per 1000 to 1 per 250,000 adults. The disease is more common in women and increases as people age. It became less common since the 1950s, with the introduction of antibiotics. It is more common among certain ethnic groups such as indigenous people.
History
René Laennec, the man who invented the stethoscope, used his invention to first discover bronchiectasis in 1819. The disease was researched in greater detail by Sir William Osler in the late 1800s; it is suspected that Osler actually died of complications from undiagnosed bronchiectasis.