
 | ||
Antiarrhythmic agents are a group of pharmaceuticals that are used to suppress abnormal rhythms of the heart (cardiac arrhythmias), such as atrial fibrillation, atrial flutter, ventricular tachycardia, and ventricular fibrillation.
Contents
- Singh Vaughan Williams classification
- Class I agents
- Class II agents
- Class III agents
- Class IV agents
- Class V other agents
- Sicilian gambit classification
- References
Many attempts have been made to classify antiarrhythmic agents. The problem arises from the fact that many of the antiarrhythmic agents have multiple modes of action, making any classification imprecise.
Singh-Vaughan Williams classification
The Singh-Vaughan Williams classification was introduced in 1970. As a doctoral candidate at Oxford University, Dr. Bramah N. Singh determined that amiodarone and sotalol had antiarrhythmic properties and belonged to a new class of antiarrhythmic agents (what would become the class III antiarrhythmic agents). Singh developed part of the classification system while working in the lab of Miles Vaughan Williams and part of the system after leaving Oxford. Singh subsequently pioneered the use of these agents at bedside over the next several decades of practice in the United States.
With regards to management of atrial fibrillation, classes I and III are used in rhythm control as medical cardioversion agents, while classes II and IV are used as rate-control agents.
The five main classes in the Singh-Vaughan Williams classification of antiarrhythmic agents are:
Class I agents
The class I antiarrhythmic agents interfere with the sodium channel. Class I agents are grouped by what effect they have on the Na+ channel, and what effect they have on cardiac action potentials.
Class I agents are called membrane-stabilizing agents. The 'stabilizing' word is used to describe the decrease of excitogenicity of the plasma membrane which is brought about by these agents. (Also noteworthy is that a few class II agents like propranolol also have a membrane stabilizing effect.)
Class I agents are divided into three groups (Ia, Ib, and Ic) based upon their effect on the length of the action potential.
Class II agents
Class II agents are conventional beta blockers. They act by blocking the effects of catecholamines at the β1-adrenergic receptors, thereby decreasing sympathetic activity on the heart. These agents are particularly useful in the treatment of supraventricular tachycardias. They decrease conduction through the AV node.
Class II agents include atenolol, esmolol, propranolol, and metoprolol.
Class III agents
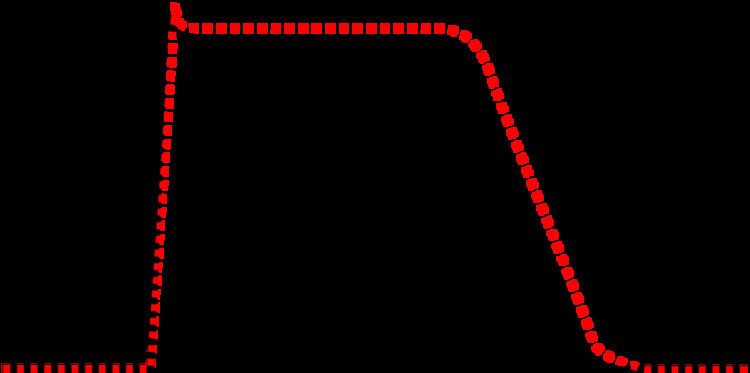
Class III agents predominantly block the potassium channels, thereby prolonging repolarization. Since these agents do not affect the sodium channel, conduction velocity is not decreased. The prolongation of the action potential duration and refractory period, combined with the maintenance of normal conduction velocity, prevent re-entrant arrhythmias. (The re-entrant rhythm is less likely to interact with tissue that has become refractory). The class III agents exhibit reverse-use dependence (their potency increases with slower heart rates, and therefore improves maintenance of sinus rhythm). Inhibiting potassium channels, slowing repolarization, results in slowed atrial-ventricular myocyte repolarization. Class III agents have the potential to prolong the QT interval of the EKG, and may be proarrhythmic (more associated with development of polymorphic VT).
Class III agents include: bretylium, amiodarone, ibutilide, sotalol, dofetilide, and dronedarone.
Class IV agents
Class IV agents are slow calcium channel blockers. They decrease conduction through the AV node, and shorten phase two (the plateau) of the cardiac action potential. They thus reduce the contractility of the heart, so may be inappropriate in heart failure. However, in contrast to beta blockers, they allow the body to retain adrenergic control of heart rate and contractility.
Class IV agents include verapamil and diltiazem.
Class V / other agents
Since the development of the original Singh-Vaughan Williams classification system, additional agents have been used that do not fit cleanly into categories I through IV.
Agents include:
Sicilian gambit classification
Another approach, known as the "Sicilian gambit", placed a greater approach on the underlying mechanism.
It presents the drugs on two axes, instead of one, and is presented in tabular form. On the Y axis, each drug is listed, in roughly the Singh-Vaughan Williams order. On the X axis, the channels, receptors, pumps, and clinical effects are listed for each drug, with the results listed in a grid. It is, therefore, not a true classification in that it does not aggregate drugs into categories.