
Specialty hematology ICD-9-CM 279.12 DiseasesDB 14176 | ICD-10 D82.0 OMIM 301000 | |
 | ||
eMedicine med/1162 ped/2443 derm/702 | ||
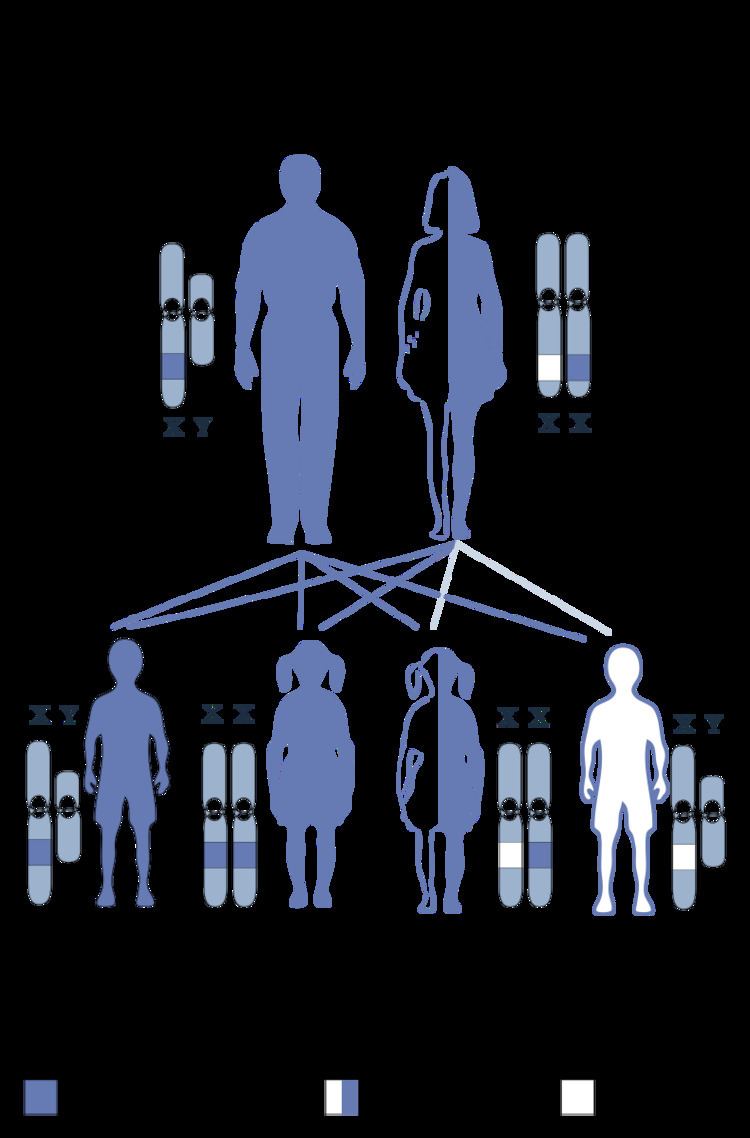
Wiskott–Aldrich syndrome (WAS) is a rare X-linked recessive disease characterized by eczema, thrombocytopenia (low platelet count), immune deficiency, and bloody diarrhea (secondary to the thrombocytopenia). It is also sometimes called the eczema-thrombocytopenia-immunodeficiency syndrome in keeping with Aldrich's original description in 1954. The WAS-related disorders of X-linked thrombocytopenia (XLT) and X-linked congenital neutropenia (XLN) may present similar but less severe symptoms and are caused by mutations of the same gene.
Contents
Signs and symptoms
The disease occurs much more in males than females (due to the X-linked recessive pattern of inheritance) and is estimated to occur in between 1 and 10 males per million. The first signs of WAS are usually petechiae and bruising, resulting from a low platelet count. Spontaneous nose bleeds and bloody diarrhea are common. Eczema develops within the first month of life. Recurrent bacterial infections develop by three months. Enlargement of the spleen is not an uncommon finding. The majority of WAS children develop at least one autoimmune disorder, and cancers (mainly lymphoma and leukemia) develop in up to a third of patients. Immunoglobulin M (IgM) levels are reduced, IgA and IgE are elevated, and IgG levels can be normal, reduced, or elevated.
Pathophysiology
In Wiskott–Aldrich syndrome, the platelets are small and do not function properly. They are removed by the spleen, which leads to low platelet counts. The immune deficiency is caused by decreased antibody production, and the inability of T cells to become polarized. This leads to increased susceptibility to infections, particularly of the ears and sinuses. T cells are unable to reorganize their actin cytoskeleton.
Genetics
Wiskott–Aldrich syndrome was linked in 1994 to mutations in a gene on the short arm of the X chromosome, which was termed Wiskott-Aldrich syndrome protein gene (WASp). The disease X-linked thrombocytopenia was later discovered to be also due to WASp mutations, but different ones from those that cause full-blown Wiskott–Aldrich syndrome. Furthermore, the rare disorder X-linked neutropenia has been linked to particular mutations of the WASp gene.
The WASp gene codes for the protein WASp, which is 502 amino acids long and is mainly expressed in hematopoietic cells (the cells in the bone marrow that develop into blood cells). The main function of WASp is to activate actin polymerization by binding to the Arp2/3 complex. In T-cells, WASp is important because it is known to be activated via T-cell receptor signaling pathways to induce cortical actin cytoskeleton rearrangements that are responsible for forming the immunological synapse.
The type of mutation to the WASp gene correlates significantly with the degree of severity: those that led to the production of a truncated protein caused significantly more symptoms than those with a missense mutation but a normal-length WASp. Although autoimmune disease and malignancy may occur in both types of mutations, those patients with truncated WASp carry a higher risk. A defect in the CD43 molecule has been found in patients with Wiskott–Aldrich syndrome.
Diagnosis
The diagnosis is made on the basis of clinical parameters, the peripheral blood smear, and low immunoglobulin levels. Typically, IgM levels are low, IgA levels are elevated, and IgE levels may be elevated; paraproteins are occasionally observed. Skin immunologic testing (allergy testing) may reveal hyposensitivity. Not all patients have a positive family history of the disorder; new mutations do occur. Often, leukemia may be suspected on the basis of low platelets and infections, and bone marrow biopsy may be performed. Decreased levels of Wiskott-Aldrich syndrome protein and/or confirmation of a causative mutation provides the most definitive diagnosis.
Sequence analysis can detect the WAS-related disorders of Wiskott–Aldrich syndrome, XLT, and XLN. Sequence analysis of the WASp gene can detect about 98% of mutations in males and 97% of mutations in female carriers. Because XLT and XLN symptoms may be less severe than full WAS and because female carriers are usually asymptomatic, clinical diagnosis can be elusive. In these cases, genetic testing can be instrumental in diagnosis of WAS-related disorders.
Classification
Jin et al. (2004) employ a numerical grading of severity:
Treatment
Treatment of Wiskott–Aldrich syndrome is currently based on correcting symptoms. Aspirin and other nonsteroidal anti-inflammatory drugs should be avoided, since these may interfere with platelet function. A protective helmet can protect children from bleeding into the brain which could result from head injuries. For severely low platelet counts, patients may require platelet transfusions or removal of the spleen. For patients with frequent infections, intravenous immunoglobulins (IVIG) can be given to boost the immune system. Anemia from bleeding may require iron supplementation or blood transfusion.
As Wiskott–Aldrich syndrome is primarily a disorder of the blood-forming tissues, a hematopoietic stem cell transplant, accomplished through a umbilical cord blood or bone marrow transplant offers the only current hope of cure. This may be recommended for patients with HLA-identical donors, matched sibling donors, or even in cases of incomplete matches if the patient is age 5 or under.
Studies of correcting Wiskott–Aldrich syndrome with gene therapy using a lentivirus have begun. Proof-of-principle for successful hematopoietic stem cell gene therapy has been provided for patients with Wiskott–Aldrich syndrome. Currently, many investigators continue to develop optimized gene therapy vectors. In July 2013 the Italian San Raffaele Telethon Institute for Gene Therapy (HSR-TIGET) reported that three children with Wiskott–Aldrich syndrome showed significant improvement 20–30 months after being treated with a genetically modified lentivirus. In April 2015 results from a follow-up British and French trial where six children with Wiskott–Aldrich syndrome were treated with gene therapy were described as promising. Median follow-up time was 27 months.
Epidemiology
The estimated incidence of Wiskott–Aldrich syndrome in the United States is one in 250,000 live male births. No geographical factor is present.
History
The syndrome is named after Dr. Robert Anderson Aldrich (1917–1998), an American pediatrician who described the disease in a family of Dutch-Americans in 1954, and Dr. Alfred Wiskott (1898–1978), a German pediatrician who first noticed the syndrome in 1937. Wiskott described three brothers with a similar disease, whose sisters were unaffected. In 2006, a German research group analysed family members of Wiskott's three cases, and surmised they probably shared a novel frameshift mutation of the first exon of the WASp gene.