
Specialty urology ICD-9-CM 593.7 MedlinePlus 000459 | ICD-10 N13.7 DiseasesDB 13835 eMedicine ped/2750 | |
 | ||
Vesicoureteral reflux (VUR) is a condition in which urine flows retrograde, or backward, from the bladder into the ureters/kidneys. Urine normally travels in one direction (forward, or anterograde) from the kidneys to the bladder via the ureters, with a 1-way valve at the ureterovesical (ureteral-bladder) junction preventing backflow. The valve is formed by oblique tunneling of the distal ureter through the wall of the bladder, creating a short length of ureter (1–2 cm) that can be compressed as the bladder fills. Reflux occurs if the ureter enters the bladder without sufficient tunneling, i.e., too "end-on."
Contents
Signs and symptoms
Most children with vesicoureteral reflux are asymptomatic. Vesicoureteral reflux may be diagnosed as a result of further evaluation of prenatal hydronephrosis or hydroureter (abnormal widening of the ureter), as well as reflux in a sibling (routine testing in either circumstance is controversial). Reflux also increases risk of urinary tract infection or acute pyelonephritis, so testing for reflux may be performed after a child has one or more infections.
In infants, the signs and symptoms of a urinary tract infection may include only fever and lethargy, with poor appetite and sometimes foul-smelling urine, while older children typically present with dysuria and frequent urination.
Causes
In healthy individuals the ureters enter the urinary bladder obliquely and run submucosally for some distance. This, in addition to the ureter's muscular attachments, helps secure and support them posteriorly. Together these features produce a valvelike effect that occludes the ureteric opening during storage and voiding of urine. In people with VUR, failure of this mechanism occurs, with resultant retrograde flow of urine.
Hardikar syndrome can include Vesicoureteral reflux, hydronephrosis, cleft lip and palate, intestinal obstruction and other symptoms.
Primary VUR
Insufficient submucosal length of the ureter relative to its diameter causes inadequacy of the valvular mechanism. This is precipitated by a congenital defect/lack of longitudinal muscle of the intravesical ureter resulting in an ureterovesicular junction (UVJ) anomaly.
Secondary VUR
In this category the valvular mechanism is intact and healthy to start with but becomes overwhelmed by raised vesicular pressures associated with obstruction, which distorts the ureterovesical junction. The obstructions may be anatomical or functional. Secondary VUR can be further divided into anatomical and functional groups.
Anatomical
Posterior urethral valves; urethral or meatal stenosis. These causes are treated surgically when possible.
Functional
Bladder instability, neurogenic bladder and non-neurogenic bladder. Urinary tract infections may cause reflux due to the elevated pressures associated with inflammation.
Resolution of functional VUR will usually occur if the precipitating cause is treated and resolved. Medical and/or surgical treatment may be indicated.
International Classification of Vesicoureteral Reflux
The younger the age of the patient and the lower the grade at presentation the higher the chance of spontaneous resolution. Most (approx. 85%) of grade I & II cases of VUR will resolve spontaneously. Approximately 50% of grade III cases and a lower percentage of higher grades will also resolve spontaneously.
Diagnosis
The following procedures may be used to diagnose VUR:
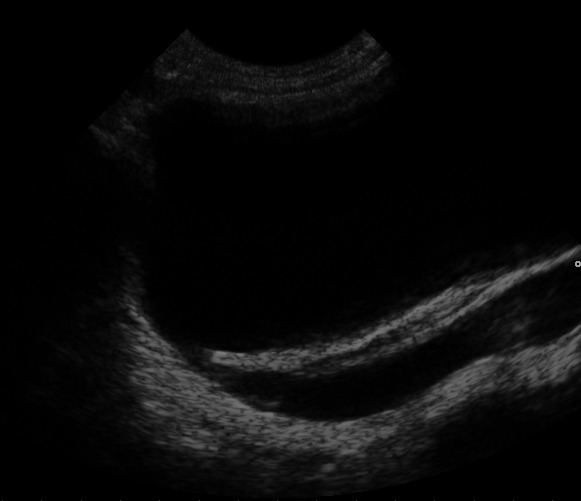
An abdominal ultrasound might suggest the presence of VUR if ureteral dilatation is present; however, in many circumstances of VUR of low to moderate, even high severity, the sonogram may be completely normal, thus providing insufficient utility as a single diagnostic test in the evaluation of children suspected of having VUR, such as those presenting with prenatal hydronephrosis or urinary tract infection (UTI).
VCUG is the method of choice for grading and initial workup, while RNC is preferred for subsequent evaluations as there is less exposure to radiation. A high index of suspicion should be attached to any case where a child presents with a urinary tract infection, and anatomical causes should be excluded. A VCUG and abdominal ultrasound should be performed in these cases
DMSA scintigraphy is used for the evaluation of the paranchymal damage, which is seen as cortical scars. After the first febrile UTI, the diagnostic role of an initial scintigraphy for detecting the damage before the VCUG was investigated and it was suggested that VCUG can be omitted in children who has no cortical scars and urinary tract dilatation.
Early diagnosis in children is crucial as studies have shown that the children with VUR who present with a UTI and associated acute pyelonephritis are more likely to develop permanent renal cortical scarring than those children without VUR, with an odds ratio of 2.8. Thus VUR not only increases the frequency of UTI's, but also the risk of damage to upper urinary structures and end-stage renal disease.
Treatment
The goal of treatment is to minimize infections, as it is infections that cause renal scarring and not the vesicoureteral reflux. Minimizing infections is primarily done by prophylactic antibiotics in newborns and infants who are not potty trained. However, in children who are older, physicians and parents should focus on bowel and bladder management. Children who hold their bladder or who are constipated have a greater number of infections than children who void on a regular schedule. When medical management fails to prevent recurrent urinary tract infections, or if the kidneys show progressive renal scarring then surgical interventions may be necessary. Medical management is recommended in children with Grade I-III VUR as most cases will resolve spontaneously. A trial of medical treatment is indicated in patients with Grade IV VUR especially in younger patients or those with unilateral disease. Of the patients with Grade V VUR only infants are trialled on a medical approach before surgery is indicated, in older patients surgery is the only option.
Endoscopic injection
Endoscopic injection involves applying a gel around the ureteral opening to create a valve function and stop urine from flowing back up the ureter. The gel consists of two types of sugar-based molecules called dextranomer and hyaluronic acid. Trade names for this combination include Deflux and Zuidex. Both constituents are well-known from previous uses in medicine. They are also biocompatible, which means that they do not cause significant reactions within the body. In fact, hyaluronic acid is produced and found naturally within the body.
Medical Treatment
Medical treatment entails low dose antibiotic prophylaxis until resolution of VUR occurs. Antibiotics are administered nightly at half the normal therapeutic dose. The specific antibiotics used differ with the age of the patient and include:
After 2 months the following antibiotics are suitable:
Urine cultures are performed 3 monthly to exclude breakthrough infection. Annual radiological investigations are likewise indicated. Good perineal hygiene, and timed and double voiding are also important aspects of medical treatment. Bladder dysfunction is treated with the administration of anticholinergics.
Surgical Management
A surgical approach is necessary in cases where a breakthrough infection results despite prophylaxis, or there is non-compliance with the prophylaxis. Similarly if the VUR is severe (Grade IV & V), there are pyelonephritic changes or congenital abnormalities. Other reasons necessitating surgical intervention are failure of renal growth, formation of new scars, renal deterioration and VUR in girls approaching puberty.
There are four types of surgical procedure available for the treatment of VUR: endoscopic (STING/HIT procedures); laparoscopic; robotic-assisted laparoscopic; and open procedures (Cohen procedure, Leadbetter-Politano procedure, Lich-Gregoir technique). Laparoscopic and robotic-assisted laparoscopic procedures are often imitation of classical open procedures in laparoscopic or robotic-assisted laparoscopic environments.
Epidemiology
It has been estimated that VUR is present in more than 10% of the population. Younger children are more prone to VUR because of the relative shortness of the submucosal ureters. This susceptibility decreases with age as the length of the ureters increases as the children grow. In children under the age of 1 year with a urinary tract infection, 70% will have VUR. This number decreases to 15% by the age of 12. Although VUR is more common in males antenatally, in later life there is a definite female preponderance with 85% of cases being female.
Follow-up
The American Urological Association recommends ongoing monitoring of children with VUR until the abnormality resolves or is no longer clinically significant. The recommendations are for annual evaluation of blood pressure, height, weight, analysis of the urine, and kidney ultrasound.