
ICD-9-CM 81.54 | ||
 | ||
Unicompartmental knee arthroplasty is a surgical procedure used to relieve arthritis in one of the knee compartments in which the damaged parts of the knee are replaced. UKA surgery may reduce post-operative pain and have a shorter recovery period than a total knee replacements. Also, UKA may have a smaller incision because the implants may be smaller.
Contents
- Background
- Indications and Contraindications
- History and physical examination
- Surgical information
- Benefits
- Risks
- Long term results
- References
In the United States, this procedure constitutes approximately 8% of knee arthroplasty.
Background
In the early 1950s, Duncan C. McKeever theorized that osteoarthritis could be isolated to only one compartment of the knee joint, and that replacement of the entire knee might not be necessary if only one knee compartment was affected. The UKA concept was designed to cause less trauma or damage than traditional total knee replacement by removing less bone and trying to maintain most of the patient’s bone and anatomy. Also, the concept was designed to use smaller implants and thereby keep most of the patient’s bone; this can help patients return to normal function faster.
Initially, UKAs were not always successful, because the implants were poorly designed, patients weren't thoroughly screened for suitability, and optimal surgical techniques were not developed. Recent advancements have been made to improve the design of the implants. Also, choosing the best-suited patients was emphasized to ensure that surgeons followed the indications and contraindications for partial replacement. Proper patient selection, following the indications/contraindications, and performing the surgery well are key factors for the success of UKA.
Currently, UKA is often referred to as "partial knee replacement." In reality there is nothing "partial" about this replacement. It is a complete replacement of the "part" of the knee that is arthritic. Patients who have arthritis restricted to only one part of the knee and have no reason to not have this surgery ("contraindications" is the medical term for a reason not to have a particular procedure) could consider this option.
Indications and Contraindications
UKA may be suitable for patients with moderate joint disease caused by painful osteoarthritis or traumatic injury, a history of unsuccessful surgical procedures or poor bone density that precludes other types of knee surgery. Patients that may not be eligible for a UKA include patients that have an active or suspected infection in or about the knee joint, may have a known sensitivity to device materials, have bone infections or disease that result in an inability to support or fixate the new implant to the bone, have inflammatory arthritis, have major deformities that can affect the knee mechanical axis, have neuromuscular disorders that may compromise motor control and/or stability, have any mental neuromuscular disorder, patients who are not skeletally mature, are obese, have lost a severe amount of bone from the shin (tibia) or have severe tibial deformities, have recurring subluxation of the knee joint, have untreated damage to the knee cap and thigh bone joint (patellofemoral joint), have untreated damage to the opposite compartment or the same side of the knee not being replaced by a device, and/or have instability of the knee ligaments such that the postoperative stability the UKA would be compromised.
The anterior cruciate ligament (ACL) should be intact, although this is debated by clinicians for patients that need a medial compartment replacement. For patients that need a lateral compartment replacement, the ACL should be intact and is contraindicated for patients that have ACL-deficient knees because the lateral component has more motion than the medial compartment.
History and physical examination
A physical examination and getting the patient’s history is performed before getting surgery. A doctor may ask the patient to identify their pain with one finger. A patient with pain in one area of the knee may be a candidate for UKA. However, a patient with pain in more than one area of the knee may not be a good candidate for UKA. The doctor may take some radiographs (e.g., x-rays) to check for degeneration of the other knee compartments and evaluate the knee. The physical exam may also include special tests designed to test the ligaments of the knee and other anatomical structures. Most likely, the surgeon will decide to do a UKA during surgery where he/she can directly see the status of the other compartments.
Surgical information
The surgeon may choose which type of incision and implant to use for the patient’s knee. During the surgery, the surgeon may align the instruments to determine the amount of bone to remove. The surgeon removes bone from the shin bone (tibia) and thigh bone (femur). The surgeon may decide to check if they removed the proper amount of bone during the surgery. In order to make sure that the proper size implant is used, a surgeon may choose to use a temporary trial. After making sure the proper size implant is selected, the surgeon will put the implant on the ends of the bone and secure it with pegs. Finally, the surgeon will close the wound with sutures.
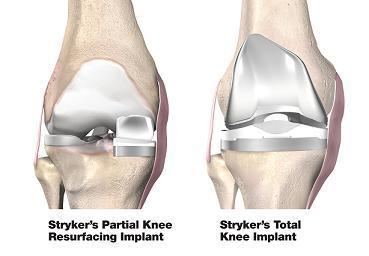
The uni-compartmental replacement is a minimally invasive option for patients whose arthritis is isolated to either the medial or the lateral compartment. The procedure offers several benefits for patients with a moderately active lifestyle, who have arthritis in just one knee compartment, and who are within normal weight ranges. The surgeon uses an incision of just 3-4 inches; a total knee replacement typically requires an incision of 8-12 inches. According to Dr. Howard J. Luks, Associate Professor of Orthopedic Surgery at New York Medical College, the partial replacement does not disrupt the knee cap, which makes for a shorter rehabilitation period. A partial replacement also causes minimal blood loss during the procedure, and results in considerably less post-operative pain. The hospitalization time compared with a total knee replacement is also greatly reduced.
Benefits
The potential benefits of UKA include a smaller incision because the UKA implants are smaller than the total knee replacements, and the surgeon may make a smaller incision. This may lead to a smaller scar. Another potential benefit is less post-operative pain because less bone is removed. Also, a quicker operation and shorter recovery period may be a result of less bone being removed during the operation and the soft tissue may sustain less trauma. Also, the rehabilitation process may be more progressive. More specific benefits of UKA are it may improve range of motion, reduce blood loss during surgery, reduce the patient’s time spent in the hospital, and decrease costs.
Currently, two of the most significant benefits of UKA or partial knee replacements are: 1. Partial knee replacement patients report that their replaced knee feels more like their original non-replaced knee as compared to a total knee replacement 2, Partial knee replacements leave other options open to further advances. By not replacing the rest of the knee with metal and plastic, if other options exist in years to come for arthritis in these areas then a partial knee replacement does not burn that bridge.
Risks
Blood clots (also known as deep vein thrombosis) are a common complication after surgery. However, a doctor may prescribe certain medications to help prevent blood clots. Infection may occur after surgery. However, antibiotics may be prescribed by a doctor to help prevent infections. Individual patient factors (e.g., anatomy, weight, prior medical history, prior joint surgeries) should be addressed with the patient’s doctor. The causes of long-term failure of UKAs include polyethylene wear, loosening of the implant, and degeneration of the adjacent knee compartment.
Long-term results
Long term studies reported excellent outcomes for UKA and the authors credit it to picking the proper patients, minimizing the amount of bone that is removed, and using the proper surgical technique. One study found that at a minimum of 10 years follow up time after the initial surgery, the overall survival rate of the implant was 96%. Also, 92% of the patients in this study had excellent or good outcome. Another study, reported that at 15 years follow up time after the initial surgery, the overall rate of the implant was 93% and 91% of these patients reported good or excellent outcomes.