
MeSH A08.340.315.350.800 TA A14.3.01.020 | Dorlands/Elsevier g_02/12384988 FMA 6469 | |
 | ||
Latin ganglion cervicothoracicum, ganglion stellatum | ||
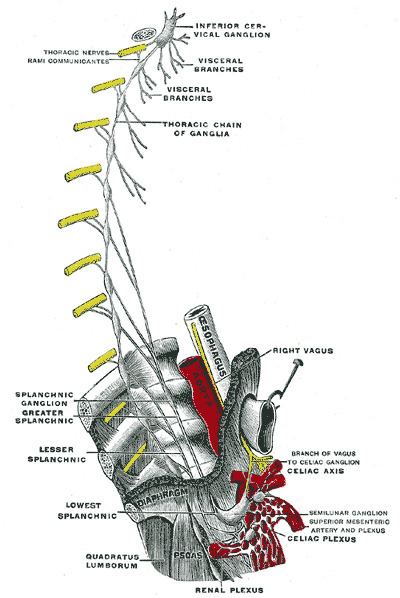
The stellate ganglion (or cervicothoracic ganglion) is a sympathetic ganglion formed by the fusion of the inferior cervical ganglion and the first thoracic ganglion, which exists in 80% of cases. Sometimes the second and the third thoracic ganglia are included in this fusion. Stellate ganglion is relatively big (10-12 x 8-20 mm) compared to much smaller thoracic, lumbar and sacral ganglia and it is polygonal in shape (lat. stellatum meaning star-shaped). Stellate ganglion is located at the level of C7, anterior to the transverse process of C7 and the neck of the first rib, superior to the cervical pleura and just below the subclavian artery. It is superiorly covered by the prevertebral lamina of the cervical fascia and anteriorly in relation with common carotid artery, subclavian artery and the beggining of vertebral artery which sometimes leaves a groove at the apex of this ganglion (this groove can sometimes even separate the stellate ganglion into so called vertebral ganglion). Relations of the apex of the stellate ganglion: • covered by the endothoracic fascia and parietal pleura • right stellate ganglion is in relation with right brachiocephalic vein anteriorly • right stellate ganglion is in relation with sternal part of subclavian artery anteriorly • laterally: first intercostal artery • medially: longus colli muscle
Contents
Clinical significance
The clinical significance of these ganglia is that they may be cut in order to decrease the symptoms exhibited by Raynaud's phenomenon and hyperhydrosis (extreme sweating) of the hands. Injection of local anesthetics near the stellate ganglion can sometimes mitigate the symptoms of sympathetically mediated pain such as complex regional pain syndrome type I (reflex sympathetic dystrophy). Injection is often given near the Chassaignac's Tubercle (anterior tubercle of transverse process of C6) due to this being an important landmark lateral to the cricoid cartilage. It is thought that anesthetic is spread along the paravertebral muscles to the stellate ganglion.
Stellate-ganglion block also shows great potential as a means of reducing the number of hot flushes and night awakenings suffered by breast cancer survivors and women experiencing extreme menopause.
Complications associated with a stellate ganglion block include Horner's syndrome, intra-arterial or intravenous injection, difficulty swallowing, vocal cord paralysis, epidural spread of local anaesthetic and pneumothorax.
Blunt needling of the stellate ganglion with an acupuncture needle is used in Traditional Chinese Medicine to decrease sympathetically mediated symptoms as well.
Block of the stellate ganglion has also been explored in coronary artery bypass surgery.
Anatomy
The stellate ganglion lies in front of the neck of the first rib. The vertebral artery lies anterior to the ganglion as it has just originated from the subclavian artery. After passing over the ganglion, the artery enters the vertebral foramen and lies posterior to the anterior tubercle of C6 (Chassaignac's Tubercle).