
ICD-10-PCS 021209W MeSH D001026 | ICD-9-CM 36.1 MedlinePlus 002946 | |
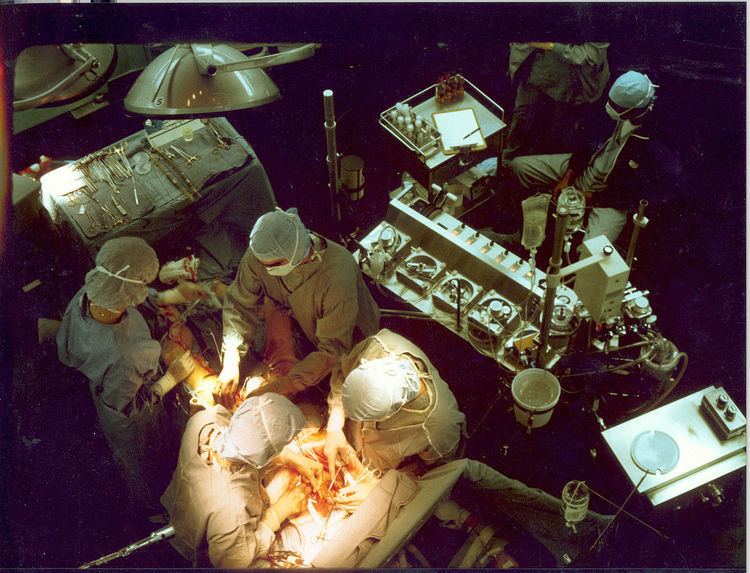 | ||
Coronary artery bypass surgery, also known as coronary artery bypass graft (CABG, pronounced "cabbage") surgery, and colloquially heart bypass or bypass surgery, is a surgical procedure to restore normal blood flow to an obstructed coronary artery.
Contents
- Terminology
- Number of arteries bypassed
- Medical uses
- Benefits
- Results compared to stent placement
- Outcomes
- CABG associated
- Open heart surgery associated
- General surgery associated
- Procedure
- Minimally invasive technique
- Choice of source of grafts
- Follow up
- Number performed
- History
- Cost
- References
There are two main approaches. In one, the left internal thoracic artery (internal mammary artery) is diverted to the left anterior descending branch of the left coronary artery. In the other, a great saphenous vein is removed from a leg; one end is attached to the aorta or one of its major branches, and the other end is attached to the obstructed artery immediately after the obstruction to restore blood flow.
It is performed to relieve angina unsatisfactorily controlled by maximum tolerated anti-ischemic medication, prevent or relieve left ventricular dysfunction, and/or reduce the risk of death. It does not prevent heart attacks. This surgery is usually performed with the heart stopped, necessitating the usage of cardiopulmonary bypass; however, two alternative techniques are also available allowing CABG to be performed on a beating heart either without using the cardiopulmonary bypass deemed as "off-pump" surgery or performing beating surgery using partial assistance of the cardiopulmonary bypass called as "on-pump beating" surgery. The latter gathers the advantages of the on-pump stopped and off-pump while minimizing their respective side-effects.
Arteries usually have a 50% to 99% obstruction. The obstruction being bypassed is due to arteriosclerosis, atherosclerosis, or both. Arteriosclerosis is characterized by thickening, loss of elasticity, and calcification of the arterial wall, most often resulting in a generalized narrowing in the affected coronary artery. Atherosclerosis is characterized by yellowish plaques of cholesterol, lipids, and cellular debris deposited into the inner layer of the wall of a large or medium-sized coronary artery, most often resulting in a focal partial obstruction in the affected artery. Each can limit blood flow if it causes a cross-sectional narrowing of at least 50%.
Terminology
There are many variations in terminology, in which one or more of "artery", "bypass" or "graft" is left out. The most frequently used acronym for this type of surgery is CABG (pronounced 'cabbage'), pluralized as CABGs (pronounced 'cabbages'). Initially the term aortocoronary bypass (ACB) was more popularly used to describe this procedure. CAGS (coronary artery graft surgery, pronounced phonetically) should not be confused with coronary angiography (CAG).
Number of arteries bypassed
The terms single bypass, double bypass, triple bypass, quadruple bypass and quintuple bypass refer to the number of coronary arteries bypassed in the procedure. In other words, a double bypass means two coronary arteries are bypassed (e.g., the left anterior descending (LAD) coronary artery and right coronary artery (RCA)); a triple bypass means three vessels are bypassed (e.g., LAD, RCA and left circumflex artery (LCX)); a quadruple bypass means four vessels are bypassed (e.g., LAD, RCA, LCX and first diagonal artery of the LAD) while quintuple means five. Left main coronary artery obstruction requires two bypasses, one to the LAD and one to the LCX. Bypass of more than four coronary arteries is uncommon.
A coronary artery may be unsuitable for bypass grafting if it is small (< 1 mm or < 1.5 mm), heavily calcified, or located within the heart muscle rather than on the surface. A single obstruction of the left main coronary artery is associated with a higher risk for a cardiac death and usually receives a double bypass.
The surgeon reviews the coronary angiogram prior to surgery and identifies the number of obstructions, the percent obstruction of each, and the suitability of the arteries beyond the obstruction(s) as targets. The presumed number of bypass grafts needed as well as the location for graft attachment is determined in a preliminary fashion prior to surgery, but the final decision as to number and location is made at surgery via direct examination of the heart.
Medical uses
Benefits
Age per se is not a factor in determining risk vs benefit of CABG.
Results compared to stent placement
CABG or stent placement is indicated when medical management - anti-anginal medications, statins, antihypertensives, smoking cessation, and /or tight blood sugar control in diabetics - do not satisfactorily relieve ischemic symptoms.
Outcomes
Prognosis following CABG depends on a variety of factors, and successful grafts typically last 8–15 years. In general, CABG improves the chances of survival of patients who are at high risk (generally triple or higher bypass), though statistically after about five years the difference in survival rate between those who have had surgery and those treated by drug therapy diminishes. Age at the time of CABG is critical to the prognosis, younger patients with no complicating diseases doing better, while older patients can usually be expected to suffer further blockage of the coronary arteries.
Grafts can become diseased and may partially or completely occlude - that is, lose their patency - in the months to years after bypass surgery is performed. A graft is considered patent if there is normal flow through the graft: flow begins to diminish with around a 70 percent stenosis in the graft.
Graft patency is dependent on a number of factors, including the type of graft used (internal thoracic artery, radial artery, or great saphenous vein), the size of the coronary artery that the graft is anastomosed with, and, of course, the skill of the surgeon(s) performing the procedure. Arterial grafts (e.g. LITA, radial) are far more sensitive to rough handling than the saphenous veins and may go into spasm if handled improperly.
Generally the best patency rates are achieved with the in-situ left internal thoracic artery (the proximal end is left connected to the subclavian artery) with the distal end being anastomosed with the coronary artery (typically the left anterior descending artery or a diagonal branch artery). Lesser patency rates can be expected with radial artery grafts and "free" internal thoracic artery grafts (where the proximal end of the thoracic artery is excised from its origin from the subclavian artery and re-anastomosed with the ascending aorta). Saphenous vein grafts have worse patency rates, but are more available, as the patients can have multiple segments of the saphenous vein used to bypass different arteries.
Veins that are used either have their valves removed or are turned around so that the valves in them do not occlude blood flow in the graft. LITA grafts are longer-lasting than vein grafts, both because the artery is more robust than a vein and because, being already connected to the arterial tree, the LITA need only be grafted at one end. The LITA is usually grafted to the left anterior descending coronary artery (LAD) because of its superior long-term patency when compared to saphenous vein grafts.
CABG associated
Open heart surgery associated
General surgery associated
Procedure
- The patient is brought to the operating room and moved onto the operating table.
- An anaesthetist or anesthesiologist places intravenous and arterial lines and injects an analgesic, usually fentanyl, intravenously, followed within minutes by an induction agent (usually propofol or etomidate) to render the patient unconscious.
- An endotracheal tube is inserted and secured by the anaesthetist and mechanical ventilation is started. General anaesthesia is maintained with an inhaled volatile anesthetic agent such as isoflurane.
- The chest is opened via a median sternotomy and the heart is examined by the surgeon.
- The bypass grafts are harvested – frequent vessels are the internal thoracic arteries, radial arteries and saphenous veins. When harvesting is done, the patient is given heparin to inhibit blood clotting.
- In the case of "off-pump" surgery, the surgeon places devices to stabilize the heart.
- In the case of "on-pump" surgery, the surgeon sutures cannulae into the heart and instructs the perfusionist to start cardiopulmonary bypass (CPB). Once CPB is established, there are two technical approaches: either the surgeon places the aortic cross-clamp across the aorta and instructs the perfusionist to deliver cardioplegia with a cooled potassium mixture to stop the heart and slow its metabolism or performing bypasses on beating state (on-pump beating).
- One end of each vein graft is sewn on to the coronary arteries beyond the obstruction and the other end is attached to the aorta or one of its branches. For the internal thoracic artery, the artery is severed and the proximal intact artery is sewn to the LAD beyond the obstruction. Aside the latter classical approach, there are emerging techniques for construction of composite grafts as to avoiding connecting grafts on the ascending aorta (Un-Aortic) in view of decreasing neurologic complications.
- The heart is restarted; or in "off-pump" surgery, the stabilizing devices are removed. In cases where the aorta is partially occluded by a C-shaped clamp, the heart is restarted and suturing of the grafts to the aorta is done in this partially occluded section of the aorta while the heart is beating.
- Protamine is given to reverse the effects of heparin.
- Chest tubes are placed in the mediastinal and pleural space to drain blood from around the heart and lungs.
- The sternum is wired together and the incisions are sutured closed.
- The patient is moved to an intensive care unit (ICU) or cardiac universal bed (CUB) to recover. Nurses in the ICU monitor blood pressure, urine output, respiratory status, and chest tubes for excessive or no drainage. Excessive drainage suggests continued bleeding which may require re-operation to manage; no drainage suggests an obstructed tube, which can result in cardiac tamponade and/or pneumothorax which can be lethal.
- After awakening and stabilizing in the ICU for 18 to 24 hours, the person is transferred to the cardiac surgery ward. If the patient is in a CUB, equipment and nursing is "stepped down" appropriate to the patient's progress without having to move the patient. Vital sign monitoring, remote rhythm monitoring, early ambulation with assistance, breathing exercises, pain control, blood sugar monitoring with intravenous insulin administration by protocol, and anti-platelet agents are all standard of care.
- The patient without complications is discharged in four or five days.
Minimally invasive technique
Alternate methods of minimally invasive coronary artery bypass surgery have been developed. Off-pump coronary artery bypass (OPCAB) is a technique of performing bypass surgery without the use of cardiopulmonary bypass (the heart-lung machine). Avoidance of aortic manipulation may be achieved through the "anaortic" or no-touch OPCAB technique, which has been shown to reduce stroke and mortality compared to on-pump CABG. Further refinements to OPCAB have resulted in minimally invasive direct coronary artery bypass surgery (MIDCAB), a technique of performing bypass surgery through a 5 to 10 cm incision.
Choice of source of grafts
The choice of vessel(s) is highly dependent upon the particular surgeon and institution. Typically, the left internal thoracic artery (LITA) (previously referred to as left internal mammary artery or LIMA) is grafted to the left anterior descending artery and a combination of other arteries and veins is used for other coronary arteries. The right internal thoracic artery (RITA), the great saphenous vein from the leg and the radial artery from the forearm are frequently used; in the U.S., these vessels are usually harvested endoscopically, using a technique known as endoscopic vessel harvesting (EVH). The right gastroepiploic artery from the stomach is infrequently used given the difficult mobilization from the abdomen.
Follow up
Number performed
CABG is one of the most common procedures performed during U.S. hospital stays; it accounted for 1.4% of all operating room procedures performed in 2011. Between 2001 and 2011, however, its volume decreased by 46%, from 395,000 operating procedures performed in 2001 to 213,700 procedures in 2011.
Between 2000 and 2012, the number of CABG procedures carried out decreased across the majority of OECD countries. However, there remained substantial variation in the rate of procedures, with the U.S. carrying out four times as many CABG operations per 100,000 people as Spain. These differences do not appear to be closely related to the incidence of heart disease, but may be due to variation in financial resources, capacity, treatment protocols and reporting methods.
History
Cost
According to the CDC, the average cost of hospitalization (only) associated with a coronary bypass operation in the United States in 2013 was $38,707, for an aggregate hospitalization cost of $6.4 billion. The International Federation of Healthcare Plans has estimated the average cost of hospitalization and physician fees for a coronary bypass operation in various countries as shown in the Table below.