
Specialty hematology DiseasesDB 12365 eMedicine article/193718 | ICD-10 D73.5 MedlinePlus 001293 MeSH D013159 | |
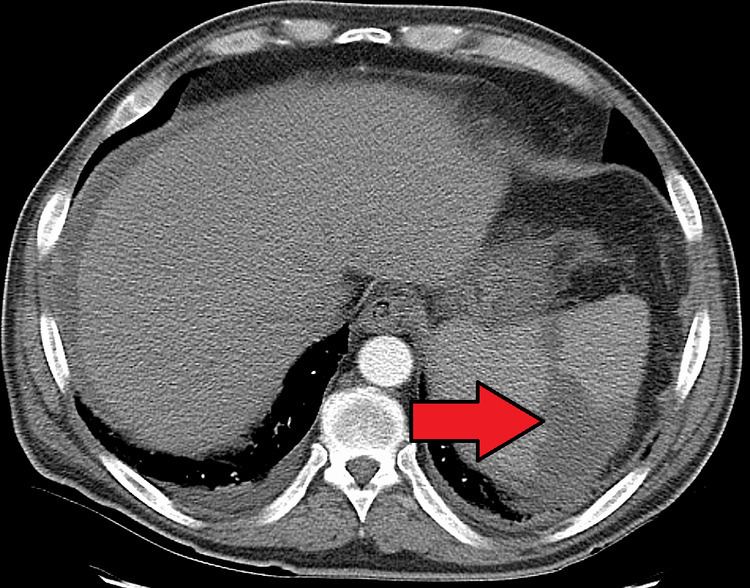 | ||
Splenic infarction is a condition in which oxygen supply to the spleen is interrupted, leading to partial or complete infarction (tissue death due to oxygen shortage) in the organ.
Contents
Splenic infarction occurs when the splenic artery or one of its branches are occluded, for example by a blood clot. Although it can occur asymptomatically, the typical symptom is severe pain in the left upper quadrant of the abdomen, sometimes radiating to the left shoulder. Fever and chills develop in some cases. It has to be differentiated from other causes of acute abdomen.
An abdominal CT scan is the most commonly used modality to confirm the diagnosis, although abdominal ultrasound can also contribute.
There is no specific treatment, except treating the underlying disorder and providing adequate pain relief. Splenectomy is only required if complications ensue; surgical removal predisposes to overwhelming post-splenectomy infections.
In one series of 59 patients, mortality amounted to 5%. Complications include a ruptured spleen, hemorrhage, splenic abscess (for example, if the underlying cause is endocarditis) or pseudocyst formation. Splenectomy may be warranted for persistent pseudocysts due to the high risk of subsequent rupture.
Causes
Several factors may increase the tendency for clot formation, such as specific infections (such as infectious mononucleosis , cytomegalovirus infection, malaria or babesiosis), inherited clotting disorders (thrombophilia, such as Factor V Leiden, antiphospholipid syndrome), malignancy (such as pancreatic cancer) or metastasis, or a combination of these factors.
In some conditions, blood clots form in one part of the circulatory system and then dislodge and travel to another part of the body, which could include the spleen. These emboligenic disorders include atrial fibrillation, patent foramen ovale, endocarditis or cholesterol embolism.
Splenic infarction is also more common in hematological disorders with associated splenomegaly, such as the myeloproliferative disorders. Other causes of splenomegaly (for example, Gaucher disease or hemoglobinopathies) can also predispose to infarction. Splenic infarction can also result from a sickle cell crisis in patients with sickle cell anemia. Both splenomegaly and a tendency towards clot formation feature in this condition. In sickle cell disease, repeated splenic infarctions lead to a non-functional spleen (autosplenectomy).
Any factor that directly compromises the splenic artery can cause infarction. Examples include abdominal traumas, aortic dissection, torsion of the splenic artery (for example, in wandering spleen) or external compression on the artery by a tumor. It can also be a complication of vascular procedures.
Splenic infarction can be due to vasculitis or diffuse intravascular coagulation. Various other conditions have been associated with splenic infarction in case reporters, for example granulomatosis with polyangiitis or treatment with drugs that predispose to vasospasm or thrombosis, like vasoconstrictors used to treat esophageal varices, sumatriptan or bevacizumab.
Therapeutic infarction
Splenic infarction can be induced for the treatment of such conditions as portal hypertension or splenic injury. It can also be used prior to splenectomy for the prevention of blood loss.