
ICD-9-CM 81.0 MedlinePlus 002968 | MeSH D013123 | |
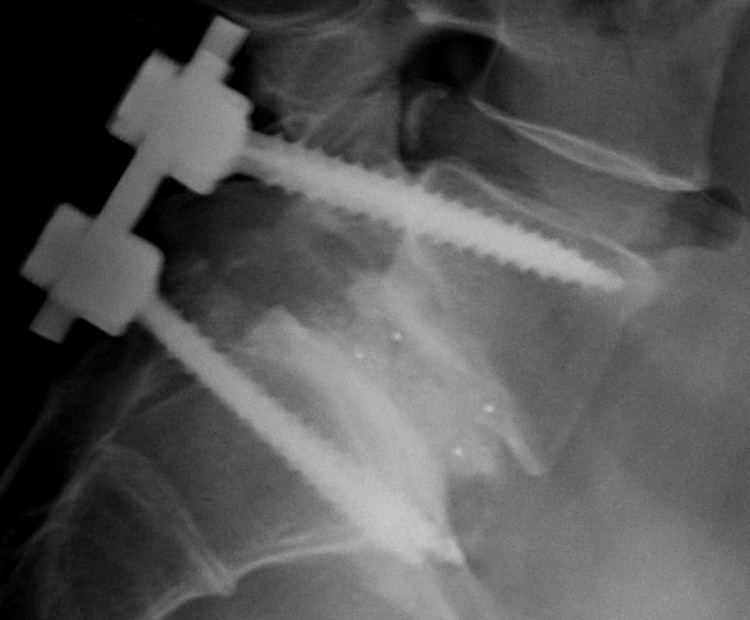 | ||
Spinal fusion, also called spondylodesis or spondylosyndesis, is a neurosurgical or orthopedic surgical technique that joins two or more vertebrae. This procedure can be performed at any level in the spine (cervical, thoracic, or lumbar) and prevents any movement between the fused vertebrae. There are many types of spinal fusion and each technique involves using bone grafting - either from the patient (autograft), donor (allograft), or artificial bone substitutes - to help the bones heal together. Additional hardware (screws, plates, or cages) is often used to hold the bones in place while the graft fuses the two vertebrae together.
Contents
- Medical uses
- Contraindications
- Epidemiology
- Costs
- Technique
- Cervical spine
- Thoracic spine
- Lumbar spine
- Risks
- During surgery
- Within a few days
- Weeks to years following surgery
- Recovery
- Frequency of use
- People who underwent spinal fusion
- References
Spinal fusion is most commonly performed to relieve the pain and pressure on the spinal cord that results when a disc (cartilage between two vertebrae) wears out (degenerative disc disease). Other common pathological conditions that are treated by spinal fusion include spinal stenosis, spondylolisthesis, spondylosis, spinal fractures, scoliosis, and kyphosis.
Like any surgery, complications may include infection, blood loss, and nerve damage. Fusion also changes the normal motion of the spine and results in more stress on the vertebrae above and below the fused segments. As a result, long-term complications include degeneration at these adjacent spine segments.
Medical uses
Spinal fusion can be used to treat a variety of conditions affecting any level of the spine - lumbar, cervical and thoracic. In general, spinal fusion is performed to decompress and stabilize the spine. The most common cause of pressure on the spinal cord/nerves is degenerative disc disease. Other common causes include disc herniation, spinal stenosis, trauma, and spinal tumors. Spinal stenosis results from bony growths (osteophytes) or thickened ligaments that cause narrowing of the spinal canal over time. This causes leg pain with increased activity, a condition called neurogenic claudication. Pressure on the nerves as they exit the spinal cord (radiculopathy) causes pain in the area where the nerves originated (leg for lumbar pathology, arm for cervical pathology). In severe cases, this pressure can cause neurologic deficits, like numbness, tingling, bowel/bladder dysfunction, and paralysis.
Lumbar and cervical spinal fusions are more commonly performed than thoracic fusions. Degeneration happens more frequently at these levels due to increased motion and stress. The thoracic spine is more immobile, so most fusions are performed due to trauma or deformities like scoliosis and kyphosis.
Conditions where spinal fusion may be considered include the following:
Contraindications
Bone morphogenetic protein (rhBMP) should not be routinely used in any type of anterior cervical spine fusion, such as with anterior cervical discectomy and fusion. There are reports of this therapy causing soft tissue swelling, which in turn can cause life-threatening complications due to difficulty swallowing and pressure on the respiratory tract.
Epidemiology
According to a report by the Agency for Healthcare Research and Quality (AHRQ), approximately 488,000 spinal fusions were performed during U.S. hospital stays in 2011 (a rate of 15.7 stays per 10,000 population), which accounted for 3.1% of all operating room procedures. This was a 70 percent growth in procedures from 2001. Lumbar fusions are the most common type of fusion performed ~ 210,000 per year. 24,000 thoracic fusions and 157,000 cervical fusions are performed each year.
A 2008 analysis of spinal fusions in the United States reported the following characteristics:
Costs
Costs associated with spinal fusion vary depending on the medical institution, insurance, type of surgery and the overall health of the patient. Total costs typically include labs, medications, room & board, medical supplies, recovery room, operating room services, physical therapy, imaging, and hospital charges. The average total hospital costs for spinal fusions increased from $24,676 in 1998 to $81,960 in 2008. The average total costs of common fusion procedures are listed below:
Technique
There are many types of spinal fusion techniques. Each technique varies depending on the level of the spine and the location of the compressed spinal cord/nerves. After the spine is decompressed, bone graft or artificial bone substitute is packed between the vertebrae to help them heal together. In general, fusions are done either on the anterior (stomach), posterior (back), or both sides of the spine. Today, most fusions are supplemented with hardware (screws, plates, rods) because they have been shown to have higher union rates than non-instrumented fusions. Minimally invasive techniques are also becoming more popular. These techniques use advanced image guidance systems to insert rods/screws into the spine through smaller incisions, allowing for less muscle damage, blood loss, infections, pain, and length of stay in the hospital. The following list gives examples of common types of fusion techniques performed at each level of the spine:
Cervical spine
Thoracic spine
Lumbar spine
- Anterior lumbar interbody fusion (ALIF) – the disc is accessed from an anterior abdominal incision
- Posterior lumbar interbody fusion (PLIF) – the disc is accessed from a posterior incision
- Transforaminal lumbar interbody fusion (TLIF) – the disc is accessed from a posterior incision on one side of the spine
- Transpsoas interbody fusion (DLIF or XLIF) – the disc is accessed from an incision through the psoas muscle on one side of the spine
- Oblique lateral lumbar interbody fusion (OLLIF) – the disc is accessed from an incision through the psoas muscle obliquely
Risks
Spinal fusion is a high risk surgery and complications can be serious, including death. In general, there is a higher risk of complications in older people with elevated body mass index (BMI), other medical problems, poor nutrition and nerve symptoms (numbness, weakness, bowel/bladder issues) before surgery. Complications also depend on the type/extent of spinal fusion surgery performed. There are three main time periods where complications typically occur:
During surgery
Within a few days
Weeks to years following surgery
Recovery
Recovery following spinal fusion is extremely variable, depending on individual surgeon's preference and the type of procedure performed. The average length of hospital stay for spinal fusions is 3.7 days. Some patients can go home the same day if they undergo a simple cervical spinal fusion at an outpatient surgery center. Minimally invasive surgeries are also significantly reducing the amount of time spent in the hospital. Recovery typically involves both restriction of certain activities and rehabilitation training. Restrictions following surgery largely depend on surgeon preference. A typical timeline for common restrictions after a lumbar fusion surgery are listed below:
Rehabilitation after spinal fusion is not mandatory. There is some evidence that it improves functional status and low back pain so some surgeons may recommend it.
Frequency of use
According to a report by the Agency for Healthcare Research and Quality (AHRQ), approximately 488,000 spinal fusions were performed during U.S. hospital stays in 2011 (a rate of 15.7 stays per 10,000 population), which accounted for 3.1% of all operating room procedures.