
Specialty Orthopedics ICD-9-CM 738.4, 756.12 DiseasesDB 12318 | ICD-10 M43.1, Q76.2 OMIM 184200 MedlinePlus 001260 | |
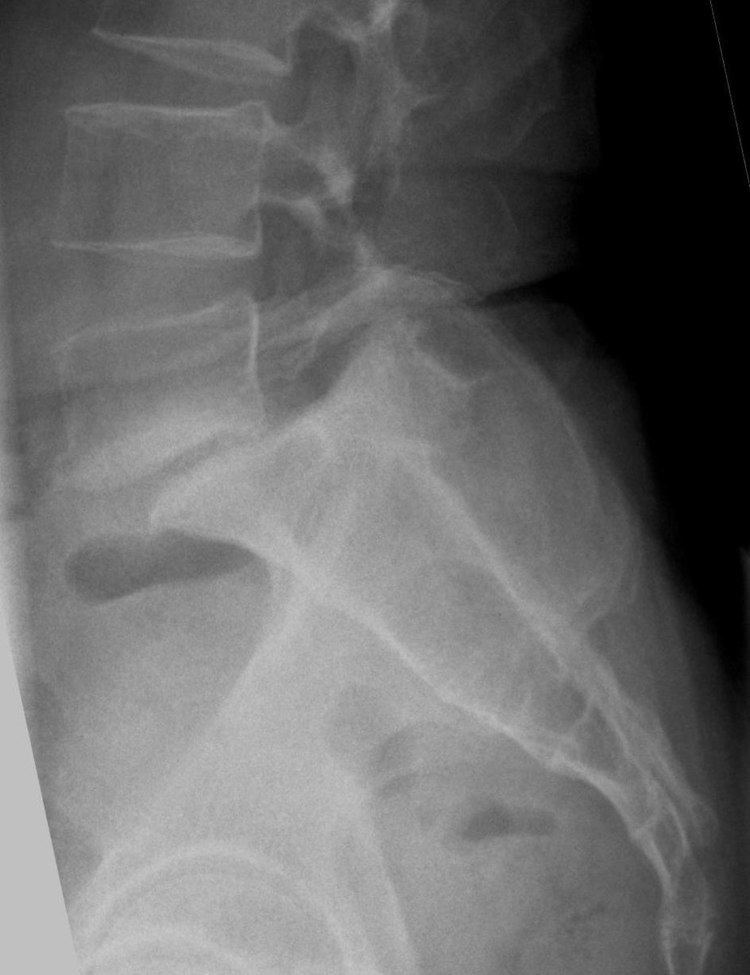 | ||
Spondylolisthesis /ˌspɒndᵻloʊlᵻsˈθiːsᵻs/ SPON-dill-oh-lis-THEE-sis is the forward or anterior displacement of one vertebra over another, and commonly involving the fifth lumbar vertebra. Backward displacement is referred to as retrolisthesis. When occurring in conjunction with scoliosis, the shortened term "olisthesis," may sometimes be used instead.
Contents
- Signs and symptoms
- Classification
- By causes
- By location
- Severity
- Conservative management
- Surgical
- History
- References
A hangman's fracture is a specific type of spondylolisthesis where the second cervical vertebra (C2) is displaced anteriorly relative to the C3 vertebra due to fractures of the C2 vertebra's pedicles.
Signs and symptoms
Symptoms of spondylolisthesis include:
Other symptoms may include tingling and numbness. Coughing and sneezing can intensify the pain. An individual may also note a "slipping sensation" when moving into an upright position. Sitting and trying to stand up may be painful and difficult.
Classification
Spondylolisthesis can be categorized by cause, location and severity.
By causes
By location
Spondylolisthesis location includes which vertebrae are involved, and may also specify which parts of the vertebrae are affected.
Isthmic spondylolisthesis is where there is a defect in the pars interarticularis. It is the most common form of spondylolisthesis; also called spondylolytic spondylolisthesis, it occurs with a reported prevalence of 5–7 percent in the US population. A slip or fracture of the intravertebral joint is usually acquired between the ages of 6 and 16 years, but remains unnoticed until adulthood. Roughly 90 percent of these isthmic slips are low-grade (less than 50 percent slip) and 10 percent are high-grade (greater than 50 percent slip). It is divided into three subtypes:
Severity
Classification by degree of the slippage, as measured as percentage of the width of the vertebral body:
Conservative management
Patients with symptomatic isthmic spondylolisthesis are initially offered conservative treatment consisting of activity modification, pharmacological intervention, and a physical therapy consultation.
Surgical
Degenerative spondylolisthesis with spinal stenosis is one of the most common indications for spine surgery (typically a laminectomy) among older adults. Both minimally invasive and open surgical techniques are used to treat spondylolisthesis.
History
Spondylolisthesis was first described in 1782 by Belgian obstetrician Herbinaux. He reported a bony prominence anterior to the sacrum that obstructed the vagina of a small number of patients. The term “spondylolisthesis” was coined in 1854 from the Greek σπονδυλος, "spondylos" = "vertebra" and ὀλισθός "olisthos" = "slipperiness," "a slip."