
Specialty hematology ICD-9-CM 285.0 DiseasesDB 12110 | ICD-10 D64.0-D64.3 OMIM 301310 206000 300751 MeSH D000756 | |
 | ||
Sideroblastic anemia or sideroachrestic anemia is a form of anemia in which the bone marrow produces ringed sideroblasts rather than healthy red blood cells (erythrocytes). In sideroblastic anemia, the body has iron available but cannot incorporate it into hemoglobin, which red blood cells need to transport oxygen efficiently. The disorder may be caused either by a genetic disorder or indirectly as part of myelodysplastic syndrome, which can evolve into hematological malignancies (especially acute myelogenous leukemia).
Contents
Sideroblasts (sidero- + -blast) are atypical, abnormal nucleated erythroblasts (precursors to mature red blood cells) with granules of iron accumulated in the mitochondria surrounding the nucleus. Normally, sideroblasts are present in the bone marrow, and enter the circulation after maturing into a normal erythrocyte.
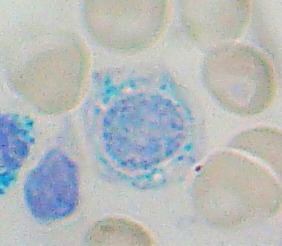
Ring sideroblasts are named so because iron-laden mitochondria form a ring around the nucleus. To count a cell as a ring sideroblast, the ring must encircle a third or more of the nucleus and contain five or more iron granules, according to the 2008 WHO classification of the tumors of the hematopoietic and lymphoid tissues.
The WHO International Working Group on Morphology of MDS (IWGM-MDS) defined three types of sideroblasts:
- Type 1 sideroblasts: fewer than 5 siderotic granules in the cytoplasm
- Type 2 sideroblasts: 5 or more siderotic granules, but not in a perinuclear distribution
- Type 3 or ring sideroblasts: 5 or more granules in a perinuclear position, surrounding the nucleus or encompassing at least one third of the nuclear circumference.
Classification
Sideroblastic anemia is typically divided into subtypes based on its cause.
GLRX5 has also been implicated.
Symptoms
Symptoms of sideroblastic anemia include skin paleness, fatigue, dizziness, and enlarged spleen and liver. Heart disease, liver damage, and kidney failure can result from iron buildup in these organs.
Causes
Causes of sideroblastic anemia can be categorized into three groups: congenital sideroblastic anemia, acquired clonal sideroblastic anemia, and acquired reversible sideroblastic anemia. All cases involve dysfunctional heme synthesis or processing. This leads to granular deposition of iron in the mitochondria that form a ring around the nucleus of the developing red blood cell. Congenital forms often present with normocytic or microcytic anemia while acquired forms of sideroblastic anemia are often normocytic or macrocytic.
Diagnosis
Ringed sideroblasts are seen in the bone marrow.
The anemia is moderate to severe and dimorphic. Microscopic viewing of the red blood cells will reveal marked unequal cell size and abnormal cell shape. Basophilic stippling is marked and target cells are common. Pappenheimer bodies are present in the red blood cells. The mean cell volume is commonly decreased (i.e., a microcytic anemia), but MCV may also be normal or even high. The RDW is increased with the red blood cell histogram shifted to the left. Leukocytes and platelets are normal. Bone marrow shows erythroid hyperplasia with a maturation arrest.
In excess of 40% of the developing erythrocytes are ringed sideroblasts. Serum iron, percentage saturation and ferritin are increased. The total iron-binding capacity of the cells is normal to decreased. Stainable marrow hemosiderin is increased.
Laboratory findings
Treatment
Occasionally, the anemia is so severe that support with transfusion is required. These patients usually do not respond to erythropoietin therapy. Some cases have been reported that the anemia is reversed or heme level is improved through use of moderate to high doses of pyrodoxine (vitamin B6). In severe cases of SBA, bone marrow transplant is also an option with limited information about the success rate. Some cases are listed on MedLine and various other medical sites. In the case of isoniazid-induced sideroblastic anemia, the addition of B6 is sufficient to correct the anemia. Desferrioxamine, a chelating agent, is used to treat iron overload from transfusions. Therapeutic phlebotomy can be used to manage iron overload.
Course and prognosis
Sideroblastic anemias are often described as responsive or non-responsive in terms of increased hemoglobin levels to pharmacological doses of vitamin B6.
1- Congenital: 80% are responsive, though the anemia does not completely resolve.
2- Acquired clonal: 40% are responsive, but the response may be minimal.
3- Acquired reversible: 60% are responsive, but course depends on treatment of the underlying cause.
Severe refractory sideroblastic anemias requiring regular transfusions and/or that undergo leukemic transformation (5-10%) significantly reduce life expectancy.