
ICD-9-CM 814.x1 | ICD-10 S62.0 | |
 | ||
eMedicine emerg/844 radio/747 plastic/318 pmr/127 | ||
A scaphoid fracture, a fracture of the scaphoid bone also known as the carpal navicular, is the most common type of carpal bone fracture. Scaphoid fractures usually cause pain at the base of the thumb accompanied by swelling in the same area. Scaphoid fractures usually cause pain and sensitivity to palpation in the anatomic snuffbox at the base of the thumb accompanied by swelling in the same area. These are also called navicular fractures (the scaphoid also being called the carpal navicular) as navicular is the traditional name for the scaphoid bone, although this can be confused with the navicular bone in the foot. Treatment depends on the location of the fracture.
Contents
Fractures of scaphoid can occur either with direct axial compression or with hyperextension of the wrist, such as a fall on the palm on an outstretched hand (FOOSH). The most common classification of scaphoid fractures categorizes them by location: distal third (distal pole), central third (waist) and proximal third (proximal pole) using the Herbert classification system.
Signs and symptoms
People with scaphoid fractures generally have snuff box tenderness. Focal tenderness is usually present in one of three places: 1) volar prominence at the distal wrist for distal pole fractures; 2) anatomic snuff box for waist or midbody fractures; 3) distal to Lister's tubercle for proximal pole fractures.
Diagnosis
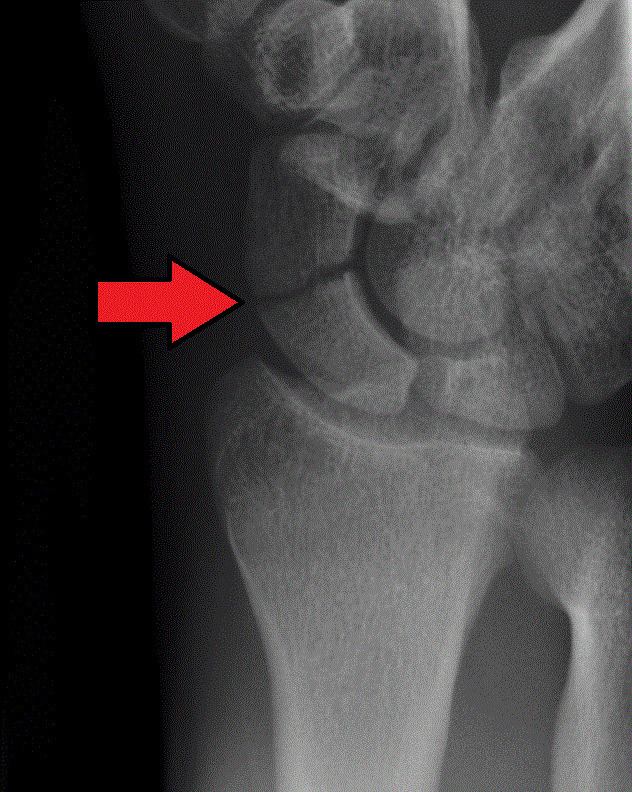
Scaphoid fractures are often diagnosed by X-rays. However, not all fractures are apparent initially. Therefore, people with tenderness over the scaphoid (those who exhibit pain to pressure in the anatomic snuff box ) are often casted for 7–10 days at which point a second set of X-rays is taken. If there was a hairline fracture, healing will now be apparent. Even then a fracture may not be apparent. A CT Scan can then be used to evaluate the scaphoid with greater resolution. Fractures can take between 6 and 12 weeks of casting to heal. The Scaphoid receives its blood supply primarily from lateral and distal branches of the radial artery. Blood flows from the top/distal end of the bone in a retrograde fashion down to the proximal pole; if this blood flow is disrupted by a fracture, the bone may not heal. Surgery is necessary at this point to mechanically mend the bone together.
The use of MRI, if available, is preferred over CT and can give one an immediate diagnosis. Bone scintigraphy is also an effective method for diagnosis fracture which do not appear on Xray.
Treatment
Treatment of scaphoid fractures is guided by the location in the bone of the fracture (proximal, waist, distal), displacement (or instability) of the fracture, and patient tolerance for cast immobilization.
Non displaced or minimally displaced waist and distal fractures have a high rate of union with closed cast management. The choice of short arm, short arm thumb spica or long arm cast is debated in the medical literature and no clear consensus or proof of the benefit of one type of casting or another has been shown; although it is generally accepted to use a short arm or short arm thumb spica for non displaced fractures. Non displaced or minimally displaced fracture can also be treated with percutaneous or minimal incision surgery which if performed correctly has a high union rate, low morbidity and faster return to activity than closed cast management. Percutaneous screw fixation is recommended over a wide surgical approach as this method preserves the palmar ligament complex and local vasculature, and helps avoid postoperative complications. This surgery includes screwing the scaphoid bone back together at the most perpendicular angle possible to promote quicker and stronger healing of the bone. During this procedure, slight excavation of the edge of the trapezium bone may be necessary to reach the scaphoid as 80% of this bone is covered with articular cartilage, which makes it difficult to gain access to the scaphoid.
Complications
Avascular necrosis (AVN) is a common complication of a scaphoid fracture. Risk of AVN depends on the location of the fracture.
Non union can also occur from undiagnosed or undertreated scaphoid fractures. Arterial flow to the scaphoid enters via the distal pole and travels to the proximal pole. This blood supply is tenuous, increasing the risk of nonunion, particularly with fractures at the wrist and proximal end. If not treated correctly non-union of the scaphoid fracture can lead to wrist osteoarthritis.
Arthritis of the wrist can occur over time due to avascular necrosis and nonunion of the scaphoid. Symptoms may include aching in the wrist, decreased range of motion of the wrist, and pain during activities such as lifting or gripping. If x-ray results show arthritis due to an old break, the treatment plan will first focus on treating the arthritis through anti-inflammatory medications and wearing a splint when an individual feels pain in the wrist. If these treatments do not help the symptoms of arthritis, steroid injections to the wrist may help alleviate pain. Should these treatments not work, surgery may be required.
Epidemiology
Fractures of the scaphoid are common in young males.