
Specialty Oncology ICD-9-CM 191 eMedicine radio/367 | ICD-10 C71 ICD-O M9421/1 MeSH D001254 | |
 | ||
Pilocytic astrocytoma or juvenile pilocytic astrocytoma or cystic cerebellar astrocytoma (and its variant juvenile pilomyxoid astrocytoma) is a brain tumor that occurs more often in children and young adults (in the first 20 years of life). They usually arise in the cerebellum, near the brainstem, in the hypothalamic region, or the optic chiasm, but they may occur in any area where astrocytes are present, including the cerebral hemispheres and the spinal cord. These tumors are usually slow growing and benign. The neoplasms are associated with the formation of a single (or multiple) cyst(s), and can become very large.
Contents
- Symptoms
- Occurrence
- Diagnosis
- Visual aspect
- Treatment
- Side effects
- Expected outcome after treatment
- References
Pilocytic astrocytomas are often cystic, and, if solid, tend to be well-circumscribed. It is characteristically easily seen on CT scans and MRI.
Juvenile pilocytic astrocytoma is associated with neurofibromatosis type 1 (NF1), and optic gliomas are among the most frequently encountered tumors in patients with this disorder. The majority of pilocytic astrocytomas have a unique KIAA1549-BRAF fusion gene.
Symptoms
Children affected by pilocytic astrocytoma can present with different symptoms that might include failure to thrive (lack of appropriate weight gain), headache, nausea, vomiting, irritability, torticollis (tilt neck or wry neck) difficulty to coordinate movements and visual complaints (including nystagmus). The complaints may vary depending on the location and size of the neoplasm. The most common symptoms are associated with increased intracranial pressure due to the size of the neoplasm.
Occurrence
According to a Dutch source juvenile pilocytic astrocytoma occurs at a rate of 2 in 100,000 people. Most affected are children ages 5–14 years.
Tumors of the optic pathway account for 3.6-6% of pediatric brain tumors, 60% of which are juvenile pilocytic astrocytomas. Astrocytomas account for 50% of pediatric primary central nervous system tumors. About 80-85% of cerebellar astrocytomas are juvenile pilocytic astrocytomas.
Recent genetic studies of pilocytic astrocytomas show that some sporadic cases have gain in chromosome 7q34 involving the BRAF locus.
Diagnosis
Usually—depending on the interview of the patient and after a clinical exam which includes a neurological exam, and an ophthalmological exam—a CT scan and or MRI scan will be performed. A special dye may be injected into a vein before these scans to provide contrast and make tumors easier to identify. The neoplasm will be clearly visible.
If a tumor is found, it will be necessary for a neurosurgeon to perform a biopsy of it. This simply involves the removal of a small amount of tumorous tissue, which is then sent to a (neuro)pathologist for examination and staging. The biopsy may take place before surgical removal of the tumor or the sample may be taken during surgery.
Visual aspect
Macroscopically, an astrocytoma is a mass that looks well-circumscribed and has a large cyst. The neoplasm may also be solid.
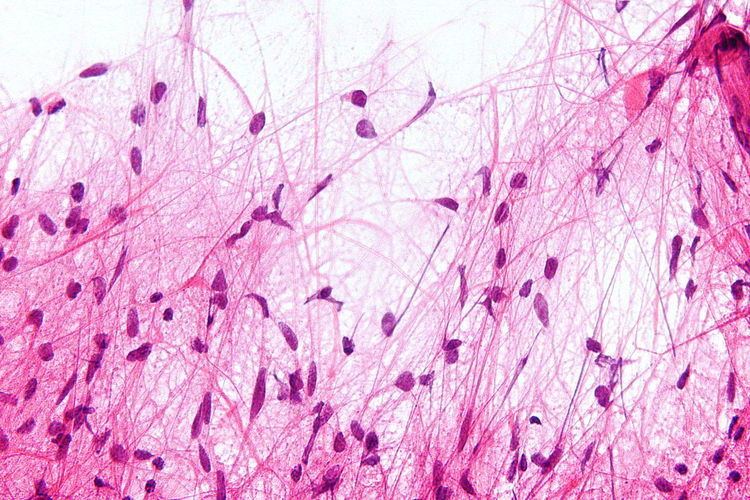
Under the microscope, the tumor is seen to be composed of bipolar cells with long "hairlike" GFAP-positive processes, giving the designation "pilocytic" (that is, made up of cells that look like fibers when viewed under a microscope). Some pilocytic astrocytomas may be more fibrillary and dense in composition. There is often presence of Rosenthal fibers, eosinophilic granular bodies and microcysts. Myxoid foci and oligodendroglioma-like cells may also be present, though non-specific. Long-standing lesions may show hemosiderin-laden macrophages and calcifications.
Treatment
Surgery is usually the treatment of choice. Total resection is often possible; however, the location could prohibit access to the neoplasm and lead to incomplete or no resection at all. Removal of the tumor will generally allow functional survival for many years. In particular for pilocytic astrocytomas (that are commonly indolent bodies that may permit normal neurologic function) surgeons may decide to monitor the neoplasm's evolution and postpone surgical intervention for some time. However, left unattended these tumors may eventually undergo neoplastic transformation.
Side effects
Children with cerebellar pilocytic astrocytoma may experience side effects related to the tumor itself and related to the treatment. Strabismus.
Expected outcome after treatment
Grade I pilocytic astrocytoma and cerebellar gliomas are not associated with recurrence after complete resection. Grade II astrocytomas and cerebellar gliomas are more likely to recur after surgical removal. Pilomyxoid astrocytomas may behave more aggressively than classic pilocytic astrocytoma.
After complete surgical removal, in cases of progressive/recurrent disease or when maximal surgical removal has been achieved, chemotherapy and/or radiation therapy will be considered by the medical team.