
To ansa cervicalis MeSH A08.800.800.120.330 FMA 50871 | Latin nervus hypoglossus TA A14.2.01.191 | |
 | ||
Innervates | ||
The hypoglossal nerve is the twelfth cranial nerve, and innervates all the extrinsic and intrinsic muscles of the tongue, except for the palatoglossus. It is solely a motor nerve. The nerve arises from the hypoglossal nucleus in the brain stem as a number of small rootlets, passes through the hypoglossal canal and down through the neck, and eventually passes up again over the tongue muscles it supplies into the tongue. There are two hypoglossal nerves in the body: one on the left, and one on the right.
Contents
The nerve is involved in controlling tongue movements required for speech and swallowing. Lesions or damage to the nerve or the neural pathways which control it can affect the ability of the tongue to move and its appearance. The name hypoglossus springs from the fact that its passage is below the tongue, hypo meaning "under", and glossus meaning "tongue", both of which are from Ancient Greek.
Structure
The hypoglossal nerve arises as a number of small rootlets from the front of the medulla, the bottom part of the brainstem, in the preolivary sulcus, which separates the olive and the pyramid. The nerve passes through the subarachnoid space and pierces the dura mater near the hypoglossal canal, an opening in the occipital bone of the skull.
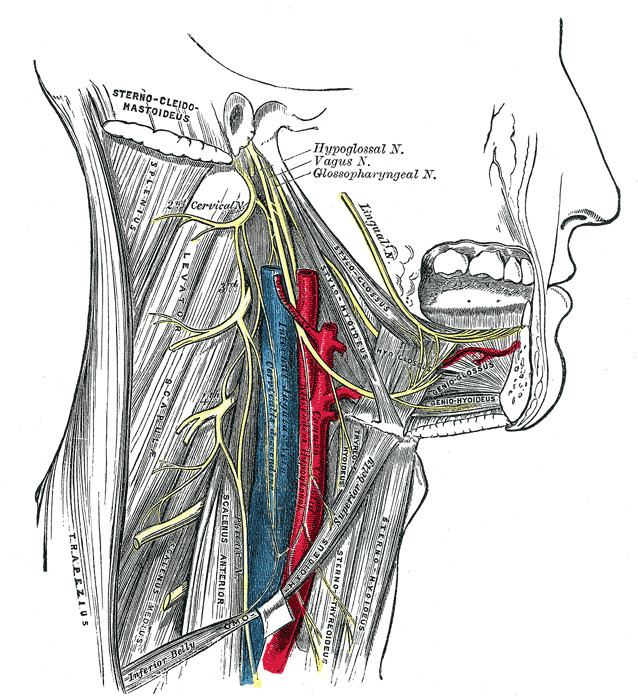
After emerging from the hypoglossal canal, the hypoglossal nerve gives off a meningeal branch and picks up a branch from the anterior ramus of C1. It then travels close to the vagus nerve and spinal division of the accessory nerve, spirals downwards behind the vagus nerve and passes between the internal carotid artery and internal jugular vein lying on the carotid sheath.
At a point at the level of the angle of the mandible, the hypoglossal nerve emerges from behind the posterior belly of the digastric muscle. It then loops around a branch of the occipital artery and travels forward into the region beneath the mandible. The hypoglossal nerve moves forward deep to the hyoglossus and stylohyoid muscles and lingual nerve. It continues deep to the genioglossus muscle and continues forward to the tip of the tongue. It distributes branches to the intrinsic and extrinsic muscle of the tongue innervates as it passes in this direction, and supplies several muscles (hyoglossus, genioglossus and stylohyoid) that it passes.
The rootlets of the hypoglossal nerve arise from the hypoglossal nucleus near the bottom of the brain stem. The hypoglossal nucleus receives input from both the motor cortices but the contralateral input is dominant; innervation of the tongue is essentially lateralized.
Signals from muscle spindles on the tongue travel through the hypoglossal nerve, moving onto the lingual nerve which synapses on the trigeminal mesencephalic nucleus.
Development
The hypoglossal nerve is derived from the first pair of occipital somites, collections of mesoderm that form next to the main axity of an embryo during development. The musculature it supplies develop as the hypoglossal cord from the myotomes of the first four four pairs of occipital somites. The nerve is first visible as a series of roots in the fourth week of development, which have formed a single nerve and link to the tongue by the fifth week.
The hypoglossal nucleus is derived from the basal plate of the embryonic medulla oblongata.
Function
The hypoglossal nerve provides motor control of the extrinsic muscles of the tongue: genioglossus, hyoglossus, styloglossus, and the intrinsic muscles of the tongue. These represent all muscles of the tongue except the palatoglossus muscle. The hypoglossal nerve is of a general somatic efferent (GSE) type.
The nerve is involved in swallowing to clear the mouth of saliva and other involuntary activities. The hypoglossal nucleus interacts with the reticular formation, involved in the control of several reflexive or automatic motions, and several corticonuclear originating fibers supply innervation aiding in unconscious movements relating to speech and articulation.
Damage
Damage or lesions to the nerve is classified according to the relation of the damage to the hypoglossal nucleus. Thus damage may be supranuclear (Latin: supra, lit. 'above'), nuclear or infranuclear (Latin: infra, lit. 'below'). Such injuries damage either an upper motor neuron (supranuclear) or the lower motor neuron (intranuclear). Damage can be on one or both sides, which will affect symptoms that the damage causes.
An injury that is supranuclear will cause the tongue to deviate away from the injured side. Such injuries can give rise to crossed symptoms due to a majority of the supranuclear innervation to the hypoglossal nucleus being crossed. This deviation will only be seen in the initial days after the injury, after which when the tongue is protruded it won't deviate, even though the nerve does not recover function. Supranuclear damage to both the left and right tracts often occurs in conjunction with damage to facial and trigeminal nerve dysfunction. This often occurs due to thrombotic damage to the brainstem following arteriosclerosis of the vertebrobasilar artery. Such a stroke may result in tight oral musculature, and difficulty speaking, eating and chewing.
Infranuclear lesions will lead to paralysis of the hypoglossal nerve leading to atrophy of muscles of the tongue. Infranuclear injuries will cause deviation of the tongue towards the affected side when it is stuck out. This is because of the weaker genioglossal muscle.
Progressive bulbar palsy, a neuromuscular atrophy associated with combined lesions of the hypoglossal nucleus and nucleus ambiguus upon atrophy of motor nerves of the pons and medulla. The symptoms are those of dysfunctional movements of the tongue leading to speech and chewing impairments, as well as swallowing difficulties, caused by dysfunction of several cranial nerve nuclei. Otherwise, the symptoms are similar to those of infranuclear lesions.
Examination
The hypoglossal nerve is tested by sticking the tongue out. If there is damage to the nerve or its pathways, the tongue will involuntarily curve to one side, due to unopposed action of the opposite genioglossus muscle. If this is the result of a lower motor neuron lesion, the tongue will curve toward the damaged side, combined with the presence of fasciculations (twitches) or atrophy. However, if the deficit is caused by an upper motor neuron lesion, the tongue will curve away from the side of the cortical damage, without the presence of either fasciculations or wasting (atrophy). Lower motor neuron damage can be to either the nerve or the nucleus. Unilateral atrophy of the muscle may be seen as a reduction in the size of the tongue on the affected side, but may also show as "wrinkling" of the tongue on the damaged side. Fasciculations may look similar to ordinary motion of the tongue, which may also be affected by tremor. For fasciculations to be indicative of neural damage they should also be present when the tongue is in a rested position, and are likened to making the tongue look like a "bag of worms".
Deviation is not always present when the nerve is damaged, and tongue strength can be tested by asking a person to poke the inside of their cheek while feeling or administering counter-pressure on the outside of the cheek. Neither is it necessary to see pronounced weakness if the damage is in the upper motor neurons, when speech difficulties may be more evident.
Weakness of the tongue is displayed as a slurring of speech. The tongue may feel "thick", "heavy", or "clumsy." Lingual sounds (i.e., l's, t's, d's, n's, r's, etc.) are slurred and this is obvious in conversation. Damage may manifest differently, and testing of posterior and anterior function of the tongue may be done through assessing ability to make a "k" or "t" sound respectively.
Use in nerve repair
The hypoglossal nerve may be connected ("anastamosed") to the facial nerve to attempt to restore function when the facial nerve is damaged. Attempts at repair by either wholly or partially connecting nerve fibres from the hypoglossal nerve to the facial nerve may be used when there is focal facial nerve damage (for example, from trauma or cancer).
History
The first recorded description of the hypoglossal nerve was by Herophilos (335–280 BC), although it was not named at the time.The first use of the name hypoglossal in Latin as nervi hypoglossi externa was used by Winslow in 1733. This was followed though by several different namings including nervi indeterminati, par lingual, par gustatorium, great sub-lingual by different authors, and gustatory nerve and lingual nerve (by Winslow). It was listed in 1778 as nerve hypoglossum magnum by Soemmering. It was then named as the great hypoglossal nerve by Cuvier in 1800 as a translation of Winslow and finally named in English by Knox in 1832.
Other animals
Development of the nerve in rodents and reptiles may give some clues as to evolutionary origins and organization of the hypoglossal nerve. Nerves supplying lingual muscles, geniohyoid and infrahyoid (or hypobranchial muscle sheet) of common embryonic origin in reptiles arise from a sustained branch of neurons reaching between the caudal medulla and level with the third cervical spinal nerves outlet. This is relevant because caudal portions of the hypoglossal nucleus are intertwined with certain motor neurons of the cervical spinal cord through the supraspinal nucleus which additionally supplies the thyrohyoid through the first spinal nerve. An organization which may be present among humans, but has not been proven occurs in rodents where the first cervical nerve has also been shown to include fibres originating from the caudal hypoglossal nucleus which pass on to innervate certain intrinsic muscles of the tongue after joining with the hypoglossal nerve somewhere along the neck.