
 | ||
The frozen section procedure is a pathological laboratory procedure to perform rapid microscopic analysis of a specimen. It is used most often in oncological surgery. The technical name for this procedure is cryosection.
Contents

The quality of the slides produced by frozen section is of lower quality than formalin fixed paraffin embedded tissue processing. While diagnosis can be rendered in many cases, fixed tissue processing is preferred in many conditions for more accurate diagnosis.
The intraoperative consultation is the name given to the whole intervention by the pathologist, which includes not only frozen section but also gross evaluation of the specimen, examination of cytology preparations taken on the specimen (e.g. touch imprints), and aliquoting of the specimen for special studies (e.g. molecular pathology techniques, flow cytometry). The report given by the pathologist is usually limited to a "benign" or "malignant" diagnosis, and communicated to the surgeon operating via intercom. When operating on a previously confirmed malignancy, the main purpose of the pathologist is to inform the surgeon if the surgical margin is clear of residual cancer, or if residual cancer is present at the surgical margin. The method of processing is usually done with the bread loafing technique. But margin controlled surgery (CCPDMA) can be performed using a variety of tissue cutting and mounting methods, including mohs surgery.
History

The frozen section procedure as practiced today in medical laboratories is based on the description by Dr Louis B. Wilson in 1905. Wilson developed the technique from earlier reports at the request of Dr William Mayo, surgeon and one of the founders of the Mayo Clinic Earlier reports by Dr Thomas S. Cullen at Johns Hopkins Hospital in Baltimore also involved frozen section, but only after formalin fixation, and pathologist Dr William Welch, also at Hopkins, experimented with Cullen's procedure but without clinical consequences. Hence, Wilson is generally credited with truly pioneering the procedure (Gal & Cagle, 2005).
Procedure

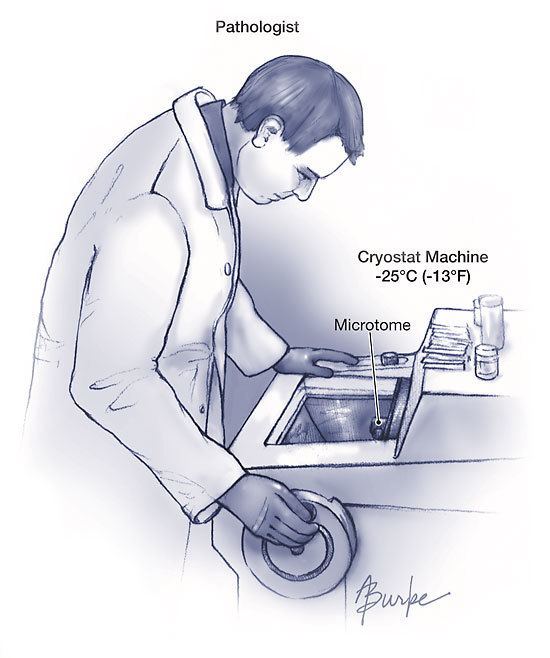
The key instrument for cryosection is the cryostat, which is essentially a microtome inside a freezer. The microtome can be compared to a very accurate "deli" slicer, capable of slicing sections as thin as 1 micrometre. The usual histology slice is cut at 5 to 10 micrometres. The surgical specimen is placed on a metal tissue disc which is then secured in a chuck and frozen rapidly to about –20 to –30 °C. The specimen is embedded in a gel like medium called OCT and consisting of poly ethylene glycol and polyvinyl alcohol; this compound is known by many names and when frozen has the same density as frozen tissue. At this temperature, most tissues become rock-hard. Usually a lower temperature is required for fat or lipid rich tissue. Each tissue has a preferred temperature for processing. Subsequently it is cut frozen with the microtome portion of the cryostat, the section is picked up on a glass slide and stained (usually with hematoxylin and eosin, the H&E stain). The preparation of the sample is much more rapid than with traditional histology technique (around 10 minutes vs 16 hours). However, the technical quality of the sections is much lower. The entire laboratory can occupy a space less than 9-square-foot (0.84 m2), and minimal ventilation is required compared to a standard wax embedded specimen laboratory.
Uses

The principal use of the frozen section procedure is the examination of tissue while surgery is taking place. This may be for various reasons:

Accuracy of diagnosis
A Cochrane systematic review published in 2016 analysed all studies that reported diagnostic accuracy of frozen sections in women undergoing surgery for suspicious tumor in ovary. The review concluded that for tumors that were clearly either benign or malignant on frozen section, the accuracy of the diagnosis was good, as confirmed later by regular biopsy. On the contrary, where the frozen section diagnosis was a borderline tumor, neither confirming not ruling out cancer, the diagnosis was less accurate. The review suggests that in such situations of uncertainty, surgeons may choose to perform additional surgery in this group of women at the time of their initial surgery in order to reduce the need for a second operation, as on an average one out of five of these women were subsequently found to have cancer.