
Latin trigonum femorale TA A04.7.03.013 | Dorlands/Elsevier 12823448 FMA 58780 | |
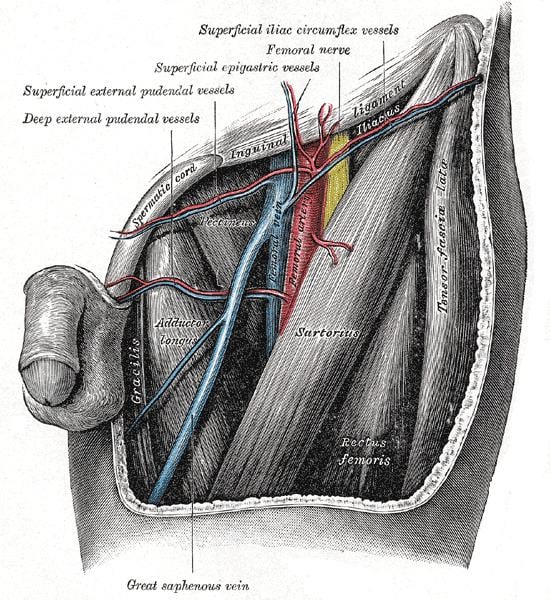 | ||
The femoral triangle (of Scarpa) is an anatomical region of the upper inner human thigh. It is a subfascial space which in living people appears as a triangular depression inferior to the inguinal ligament when the thigh is flexed, abducted and laterally rotated.
Contents
Structure
The femoral triangle is bounded:
Its floor is formed by the pectineus and adductor longus muscles medially and iliopsoas muscle laterally. Its roof is formed by the fascia lata, except at the saphenous opening where it is formed by the cribriform fascia.
Contents
The femoral triangle is important as a number of vital structures pass through it, right under the skin. The following structures are contained within the femoral triangle (from lateral to medial):
Clinical significance
Since the femoral triangle provides easy access to a major artery, coronary angioplasty and peripheral angioplasty is often performed by entering the femoral artery at the femoral triangle. Heavy bleeding in the leg can be stopped by applying pressure to points in the femoral triangle. Another clinical significance of the femoral triangle is that the femoral artery is positioned at the midinguinal point (midpoint between the pubic symphysis and the anterior superior iliac spine); medial to it lies the femoral vein. Thus the femoral vein, once located, allows for femoral venipuncture.. Femoral venopuncture is useful when there are no superficial veins that can be aspirated in a patient, in the case of collapsed veins in other parts of body (e.g. arms). The positive pulsation of the femoral artery signifies that the heart is beating and also blood is flowing to the lower extremity.
It is also necessary to appreciate clinically that this is a case where the nerve is more lateral than the vein. In most other cases the nerve (relative to its associated artery and vein) would be the deepest or more medial followed by the artery and then the vein. But in this case it is the opposite. This must be remembered when venous or arterial samples are required from the femoral vessels.
This area contains the superficial and deep basins of the inguinal lymph nodes, and is the location targeted in an inguinal lymphadenectomy. The basins are separated by the fascia lata. For patients with palpable nodal disease, removal of the superficial and deep basins are recommended. In a patient with a positive sentinel lymph node biopsy, generally only the superficial nodes are removed, unless Cloquet's node (the most superior of the deep nodes) is clinically positive.