
ICD-9-CM 347 Patient UK Cataplexy | ICD-10 G47.4 DiseasesDB 16311 MeSH D002385 | |
 | ||
Cataplexy is a sudden and transient episode of muscle weakness accompanied by full conscious awareness, typically triggered by emotions such as laughing, crying, or terror. It is the cardinal symptom of narcolepsy with cataplexy affecting roughly 70% of people who have narcolepsy, and is caused by an autoimmune destruction of the neurotransmitter hypocretin (also called orexin), which regulates arousal and wakefulness. Cataplexy without narcolepsy is rare and the cause is unknown.
Contents
- Signs and symptoms
- Mechanism
- Theories for episodes
- Hypocretin
- Diagnosis
- Treatment
- Gamma hydroxybutyrate
- Antidepressants
- Research
- References
The term cataplexy originates from the Greek κατά (kata, meaning "down"), and πλῆξις (plēxis, meaning "stroke").
Signs and symptoms
Cataplexy manifests itself as muscular weakness which may range from a barely perceptible slackening of the facial muscles to complete muscle paralysis with postural collapse. Attacks are brief, most lasting from a few seconds to a couple of minutes, and typically involve dropping of the jaw, neck weakness, and/or buckling of the knees. Even in a full-blown collapse, people are usually able to avoid injury because they learn to notice the feeling of the cataplectic attack approaching and the fall is usually slow and progressive. Speech may be slurred and vision may be impaired (double vision, inability to focus), but hearing and awareness remain normal.
Cataplexy attacks are self-limiting and resolve without the need for medical intervention. If the person is reclining comfortably, he or she may transition into sleepiness, hypnagogic hallucinations, or a sleep-onset REM period. While cataplexy worsens with fatigue, it is different from narcoleptic sleep attacks and is usually, but not always, triggered by strong emotional reactions such as laughter, anger, surprise, awe, and embarrassment, or by sudden physical effort, especially if the person is caught off guard. One well known example of this was the reaction of 1968 Olympic long jump medalist Bob Beamon on understanding that he had broken the previous world record by over 0.5 meters (2 feet). Cataplectic attacks may also occur spontaneously with no identifiable emotional trigger.
Mechanism
Cataplexy is considered secondary when it is due to specific lesions in the brain that cause a depletion of the hypocretin neurotransmitter. Secondary cataplexy is associated with specific lesions located primarily in the lateral and posterior hypothalamus. Cataplexy due to brainstem lesions is uncommon particularly when seen in isolation. The lesions include tumors of the brain or brainstem and arterio-venous malformations. Some of the tumors include astrocytoma, glioblastoma, glioma, and subependynoma. These lesions can be visualized with brain imaging, however in their early stages they can be missed. Other conditions in which cataplexy can be seen include ischemic events, multiple sclerosis, head injury, paraneoplastic syndromes, and infections such as encephalitis. Cataplexy may also occur transiently or permanently due to lesions of the hypothalamus that were caused by surgery, especially in difficult tumor resections. These lesions or generalized processes disrupt the hypocretin neurons and their pathways. The neurological process behind the lesion impairs pathways controlling the normal inhibition of muscle tone drop, consequently resulting in muscle atonia.
Theories for episodes
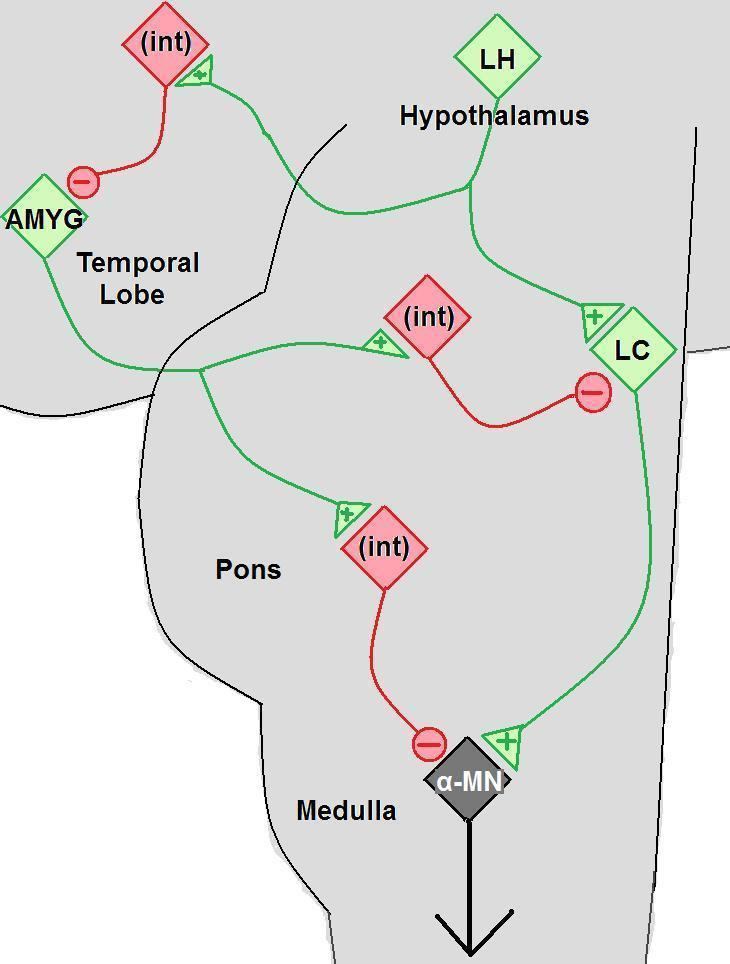
A phenomenon of REM sleep, muscular paralysis, occurs at an inappropriate time. This loss of tonus is caused by massive inhibition of motor neurons in the spinal cord. When this happens during waking, the victim of a cataplectic attack loses control of his or her muscles. As in REM sleep, the person continues to breathe and is able to control eye movements.
Hypocretin
The hypothalamus region of the brain regulates basic functions of hormone release, emotional expression and sleep. A study in 2006 in "Tohoku Journal of Experimental Medicine" concluded that the neurochemical hypocretin, which is regulated by the hypothalamus, was significantly reduced in study participants with symptoms of cataplexy. Orexin, also known as Hypocretin, is a primary chemical important in regulating sleep as well as states of arousal. Hypocretin deficiency is further associated with decreased levels of histamine and epinephrine, which are chemicals important in promoting wakefulness, arousal and alertness.
Diagnosis
The diagnosis of narcolepsy and cataplexy is usually made by symptom presentation. Presenting with the tetrad of symptoms (Excessive daytime sleepiness, sleep onset paralysis, hypnogogic hallucinations, cataplexy symptoms) is strong evidence of the diagnosis of narcolepsy. A Multiple Sleep Latency Test (MSLT) is often conducted in order to quantify daytime sleepiness.
Treatment
Cataplexy is treated with medications. There are no behavioral treatments. People with narcolepsy will often try to avoid thoughts and situations that they know are likely to evoke strong emotions because they know that these emotions are likely to trigger cataplectic attacks.
Gamma-hydroxybutyrate
Sodium oxybate and gamma-hydroxybutyrate has been found to be effective at reducing the number of cataplexy episodes. Sodium oxybate is generally safe. Sodium oxybate is typically the recommended treatment.
Antidepressants
If the above treatment is not possible venlafaxine is recommended. Evidence for benefit is not as good.
Previous treatments include tricyclic antidepressants such as imipramine, clomipramine or protriptyline. Monoamine oxidase inhibitors may be used to manage both cataplexy and the REM sleep-onset symptoms of sleep paralysis and hypnagogic hallucinations.
Research
Research is being conducted on hypocretin gene therapy and hypocretin cell transplantation for narcolepsy-cataplexy.