
ICD-9-CM 746.89 DiseasesDB 31999 | ICD-10 I49.8 OMIM 601144 eMedicine med/3736 | |
 | ||
Brugada syndrome (BrS) is a genetic disease that is characterised by abnormal electrocardiogram (ECG) findings and an increased risk of sudden cardiac death. It is named for the Spanish cardiologists Pedro Brugada, Josep Brugada and Ramon Brugada. It is the major cause of sudden unexplained death syndrome (SUDS), also known as sudden adult death syndrome (SADS), and is the most common cause of sudden death in young men without known underlying cardiac disease in Thailand and Laos.
Contents
Although the ECG findings of Brugada syndrome were first reported among survivors of cardiac arrest in 1989, it was only in 1992 that the Brugada brothers recognized it as a distinct clinical entity, causing sudden death by causing ventricular fibrillation (a potentially lethal arrhythmia) in the heart.
Genetics
Approximately 20% of the cases of Brugada syndrome have been shown to be associated with mutations in a gene that encodes for a sodium ion channel in the cell membranes of the muscle cells of the heart (the myocytes); this is often referred to as a sodium channelopathy. The majority of patients affected by Brugada syndrome are not found to have known genetic mutations to explain the disease, as of 2015. The gene, named SCN5A, is located on the short arm of the third chromosome (3p21). Loss-of-function mutations in this gene lead to a loss of the action potential dome of some epicardial areas of the right ventricle. This results in transmural and epicardial dispersion of repolarization. The transmural dispersion underlies ST-segment elevation and the development of a vulnerable window across the ventricular wall, whereas the epicardial dispersion of repolarization facilitates the development of phase 2 reentry, which generates a phase 2 reentrant extrasystole that captures the vulnerable window to precipitate ventricular tachycardia and/or ventricular fibrillation that often results in sudden cardiac death. At present time however, all the reported patients who died because of the disease and were submitted to detailed autopsy study have shown a structural right ventricular pathology underlying the syndrome.
Over 160 mutations in the SCN5A gene have been discovered to date, each having varying mechanisms and effects on function, thereby explaining the varying degrees of likelihood of the genetic mutation leading to the disease ( that is to say, penetrance) and expression of this disorder.
An example of one of the mechanisms in which a loss of function of the sodium channel occurs is a mutation in the gene that disrupts the sodium channel's ability to bind properly to ankyrin-G, an important protein mediating interaction between ion channels and cytoskeletal elements. Very recently a mutation in a second gene, Glycerol-3-phosphate dehydrogenase 1-like gene (GPD1L) has been shown to result in Brugada syndrome in a large multigenerational family (London, 2006). This gene acts as an ion channel modulator in the heart, although the exact mechanism is not yet understood.
Recently Antzelevitch has identified mutations in the L-type calcium channel subunits (CACNA1C (A39V and G490R) and CACNB2 (S481L)) leading to ST elevation and a relatively short QT interval (below 360 ms). For a comprehensive list of all mutations see In 2013, Bezzina et al. showed that common variants at SCN5A-SCN10A and HEY2 are associated with Brugada syndrome.
This condition is inherited in an autosomal dominant pattern and manifests itself more commonly in males, due to a higher penetrance. In addition it has a higher prevalence in most Asian populations.
Prevalence
The prevalence of Brugada ECG is indeed higher in Asia than in the United States and Europe. Specifically, Brugada Type 1 ECG appears more frequently in Asia (0%–0.36% of the population) and Europe (0%–0.25%) than in the United States (0.03%). Type 2 and Type 3 ECG is more prevalent in Asia (0.12%–2.23%) than in Europe (0.0%–0.6%) or the United States (0.02%).
Diagnosis
Genetic testing for Brugada syndrome is clinically available and may help confirm a diagnosis, as well as differentiate between relatives who are at risk for the disease and those who are not. Some symptoms when pinpointing this disease include fainting, irregular heartbeats, and chaotic heartbeats. However, just detecting the irregular heartbeat may be a sign of another disease, so the doctor must detect another symptom as well.
Electrocardiography
In some cases, the disease can be detected by observing characteristic patterns on an electrocardiogram. These patterns may be present all the time, they might be elicited by the administration of particular drugs (e.g., Class IA, such as ajmaline or procainamide, or class 1C, such as flecainide or pilsicainide, antiarrhythmic drugs that block sodium channels and cause appearance of ECG abnormalities), or they might resurface spontaneously due to as-yet unclarified triggers.
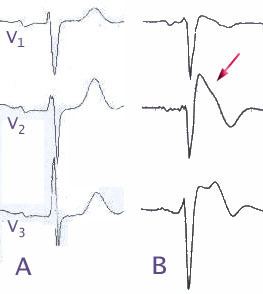
Brugada syndrome has three different ECG patterns:
The pattern seen on the ECG is persistent ST elevations in the electrocardiographic leads V1-V3 with a right bundle branch block (RBBB) appearance, with or without the terminal S waves in the lateral leads that are associated with a typical RBBB. A prolongation of the PR interval (a conduction disturbance in the heart) is also frequently seen. The ECG can fluctuate over time, depending on the autonomic balance and the administration of antiarrhythmic drugs. Adrenergic stimulation decreases the ST segment elevation, while vagal stimulation worsens it. (There is a case report of a patient who died while shaving, presumed due to the vagal stimulation of the carotid sinus massage.)
The administration of class Ia, Ic, and III drugs increases the ST segment elevation, as does fever. Exercise decreases ST segment elevation in some patients, but increases it in others (after exercise, when the body temperature has risen). The changes in heart rate induced by atrial pacing are accompanied by changes in the degree of ST segment elevation. When the heart rate decreases, the ST segment elevation increases, and when the heart rate increases, the ST segment elevation decreases. However, the contrary can also be observed.
Treatment
The cause of sudden death in Brugada syndrome is ventricular fibrillation (VF). The average age of death is 41. According to clinical reports, sudden death in people with Brugada syndrome most often happens during sleep. The episodes of syncope (fainting) and sudden death (aborted or not) are caused by fast polymorphic ventricular tachycardias or ventricular fibrillation. These arrhythmias appear with no warning. While there is no exact treatment modality that reliably and totally prevents ventricular fibrillation from occurring in this syndrome, treatment lies in termination of this lethal arrhythmia before it causes death. This is done via insertion of an implantable cardioverter-defibrillator (ICD), which continuously monitors the heart rhythm and will shock the wearer if ventricular fibrillation is sensed.
Recent studies have evaluated the role of quinidine, a Class Ia antiarrhythmic drug, for decreasing VF episodes occurring in this syndrome. Quinidine has been found to both decrease the number of VF episodes and correct spontaneous ECG changes, possibly via inhibiting Ito channels. Some drugs have been reported to induce the type-1 ECG and/or (fatal) arrhythmias in Brugada syndrome patients. Patients with Brugada syndrome can prevent arrhythmias by avoiding these drugs or using them only in controlled conditions. Those with risk factors for coronary artery disease may require an angiogram before ICD implantation.