
ICD-9-CM 007.8 MeSH D016776 | DiseasesDB 33233 | |
 | ||
Blastocystosis refers to a medical condition caused by infection with Blastocystis. Blastocystis is a protozoal, single-celled parasite that inhabits the gastrointestinal tracts of humans and other animals. Many different types of Blastocystis exist, and they can infect humans, farm animals, birds, rodents, amphibians, reptiles, fish, and even cockroaches.
Contents
Classification
There are conflicting reports regarding whether Blastocystis causes disease in humans. These reports resulted in a brief debate in medical journals in the early 1990s between some physicians in the United States who believed that Blastocystis was harmless, and physicians in the United States and overseas who believed it could cause disease.
At the time, it was common practice to identify all Blastocystis from humans as Blastocystis hominis, while Blastocystis from animals was identified differently (e.g. Blastocystis ratti from rats). Research performed since then has shown that the concept of Blastocystis hominis as a unique species of Blastocystis infecting humans is not supported by microbiological findings. Although one species group associated with primates was found, it was also discovered that humans can acquire infection from any one of nine species groups of Blastocystis which are also carried by cattle, pigs, rodents, chickens, pheasants, monkeys, dogs and other animals. Research has suggested that some types produce few or no symptoms, while others producing illness and intestinal inflammation. Researchers have suggested conflicting reports may be due to the practice of naming all Blastocystis from humans Blastocystis hominis and have proposed discontinuing the use of that term.
A standard naming system for Blastocystis organisms from humans and animals has been proposed which names Blastocystis isolates according to the genetic identity of the Blastocystis organism rather than the host. The naming system used identifies all isolates as Blastocystis sp. subtype nn where nn is a number from 1 to 9 indicating the species group of the Blastocystis organism. The identification of the species can not be performed with a microscope at this time, because the different species look alike. Identification requires equipment for genetic analysis that is common in microbiology laboratories, but not available to most physicians. Some new scientific papers have begun using the standard naming system.
Signs and symptoms
Researchers have published conflicting reports concerning whether Blastocystis causes symptoms in humans, with one of the earliest reports in 1916. The incidence of reports associated with symptoms began to increase in 1984, with physicians from Saudi Arabia reporting symptoms in humans and US physicians reporting symptoms in individuals with travel to less developed countries. A lively debate ensued in the early 1990s, with some physicians objecting to publication of reports that Blastocystis caused disease. Some researchers believe the debate has been resolved by finding of multiple species of Blastocystis that can infect humans, with some causing symptoms and others being harmless (see Genetics and Symptoms).
A few of most commonly reported symptoms are:
Some less commonly reported symptoms include:
Variation in severity
Researchers have sought to develop models to understand the variety of symptoms seen in humans. Some patients do not have symptoms, while others report severe diarrhea and fatigue.
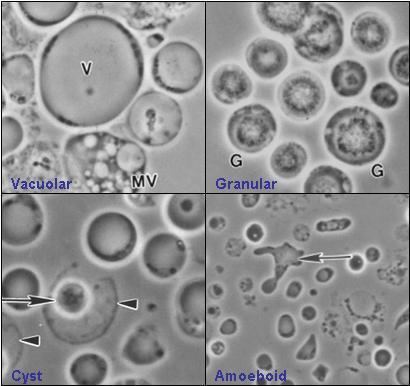
A number of researchers have investigated the possibility that some species of Blastocystis are more virulent than others. An Italian researcher reported differences in the protein profiles of isolates associated with chronic and acute infection. A research team from Malaysia reported that isolates from symptomatic patients produced large amoeboid forms that were not present in isolates from asymptomatic patients. The development of a classification system for Blastocystis in 2007 produced a series of studies investigating this possibility.
The studies that followed generally found that there is no specific "pathogenic" or non-pathogenic species of Blastocystis. One study investigated the subtypes found in patients with irritable bowel syndrome (IBS), inflammatory bowel disease (IBD), and chronic diarrhea, and found the subtypes in these diseases were similar (subtypes 2 and 3), and have also been found in asymptomatic carriers. The researchers concluded that host factors, such as age and genetics, may play the dominant role in determining the symptoms seen in the disease.
Associations
The following reports have linked Blastocystis infection to irritable bowel syndrome:
The following reports have linked Blastocystis infection to inflammatory bowel disease:
Clinically available
Diagnosis is performed by determining if the infection is present, and then making a decision as to whether the infection is responsible for the symptoms. Diagnostic methods in clinical use have been reported to be of poor quality and more reliable methods have been reported in research papers.
For identification of infection, the only method clinically available in most areas is the Ova and Parasite (O&P) exam, which identifies the presence of the organism by microscopic examination of a chemically preserved stool specimen. This method is sometimes called "Direct Microscopy". In the United States, pathologists are required to report the presence of Blastocystis when found during an O&P exam, so a special test does not have to be ordered. Direct Microscopy is inexpensive, as the same test can identify a variety of gastrointestinal infections, such as Giardia, Entamoeba histolytica, Cryptosporidium. However one laboratory director noted that pathologists using conventional microscopes failed to identify many Blastocystis infections, and indicated the necessity for special microscopic equipment for identification. The following table shows the sensitivity of Direct Microscopy in detecting Blastocystis when compared to stool culture, a more sensitive technique. Stool culture was considered by some researchers to be the most reliable technique, but a recent study found stool culture only detected 83% of individuals infected when compared to polymerase chain reaction (PCR) testing.
Reasons given for the failure of Direct Microscopy include: (1) Variable Shedding: The quantity of Blastocystis organisms varies substantially from day to day in infected humans and animals; (2) Appearance: Some forms of Blastocystis resemble fat cells or white blood cells, making it difficult to distinguish the organism from other cells in the stool sample; (3) Large number of morphological forms: Blastocystis cells can assume a variety of shapes, some have been described in detail only recently, so it is possible that additional forms exist but have not been identified.
Several methods have been cited in literature for determination of the significance of the finding of Blastocystis:
- Diagnosis only when large numbers of organism present: Some physicians consider Blastocystis infection to be a cause of illness only when large numbers are found in stool samples. Researchers have questioned this approach, noting that it is not used with any other protozoal infections, such as Giardia or Entamoeba histolytica. Some researchers have reported no correlation between number of organisms present in stool samples and the level of symptoms. A study using polymerase chain reaction testing of stool samples suggested that symptomatic infection can exist even when sufficient quantities of the organism do not exist for identification through Direct Microscopy.
- Diagnosis-by-exclusion: Some physicians diagnose Blastocystis infection by excluding all other causes, such as infection with other organisms, food intolerances, colon cancer, etc. This method can be time consuming and expensive, requiring many tests such as endoscopy and colonoscopy.
- Disregarding Blastocystis : In the early to mid-1990s, some US physicians suggested all findings of Blastocystis are insignificant. No recent publications expressing this opinion could be found.
Not clinically available
The following diagnostic methods are not routinely available to patients. Researchers have reported that they are more reliable at detecting infection, and in some cases can provide the physician with information to help determine whether Blastocystis infection is the cause of the patient's symptoms:
Serum antibody testing: A 1993 research study performed by the NIH with United States patients suggested that it was possible to distinguish symptomatic and asymptomatic infection with Blastocystis using serum antibody testing. The study used blood samples to measure the patient's immune reaction to chemicals present on the surface of the Blastocystis cell. It found that patients diagnosed with symptomatic Blastocystis infection exhibited a much higher immune response than controls who had Blastocystis infection but no symptoms. The study was repeated in 2003 at Ain Shams University in Egypt with Egyptian patients with equivalent results.
Fecal antibody testing: A 2003 study at Ain Shams University in Egypt indicated that patients symptomatically infected could be distinguished with a fecal antibody test. The study compared patients diagnosed with symptomatic Blastocystis infection to controls who had Blastocystis infection but no symptoms. In the group with symptoms, IgA antibodies to Blastocystis were detected in fecal specimens that were not present in the healthy control group.
Stool culture: Culturing has been shown to be a more reliable method of identifying infection. In 2006, researchers reported the ability to distinguish between disease causing and non-disease causing isolates of Blastocystis using stool culture. Blastocystis cultured from patients who were sick and diagnosed with Blastocystis infection produced large, highly adhesive amoeboid forms in culture. These cells were absent in Blastocystis cultures from healthy controls. Subsequent genetic analysis showed the Blastocystis from healthy controls was genetically distinct from that found in patients with symptoms. Protozoal culture is unavailable in most countries due to the cost and lack of trained staff able to perform protozoal culture.
Genetic analysis of isolates: Researchers have used techniques which allow the DNA of Blastocystis to be isolated from fecal specimens. This method has been reported to be more reliable at detecting Blastocystis in symptomatic patients than stool culture. This method also allows the species group of Blastocystis to be identified. Research is continuing into which species groups are associated with symptomatic (see Genetics and Symptoms) blastocystosis.
Immuno-fluorescence (IFA) stain: An IFA stain causes Blastocystis cells to glow when viewed under a microscope, making the diagnostic method more reliable. IFA stains are in use for Giardia and Cryptosporidium for both diagnostic purposes and water quality testing. A 1991 paper from the NIH described the laboratory development of one such stain. However, no company currently offers this stain commercially.
Transmission and risk factors
Humans contract Blastocystis infection by drinking water or eating food contaminated with feces from an infected human or animal. Blastocystis infection can be spread from animals to humans, from humans to other humans, from humans to animals, and from animals to animals. Risk factors for infection have been reported as following:
Research studies have suggested the following items are not risk factors for contracting Blastocystis infection:
Pathogeneses
Pathogenesis refers to the mechanism by which an organism causes disease. The following disease-causing mechanisms have been reported in studies of Blastocystis infection:
Treatment
There is a lack of scientific study to support the efficacy of any particular treatment. An additional review published in 2009 made a similar conclusion, noting that because the diagnostics in use have been unreliable, it has been impossible to determine whether a drug has eradicated the infection, or just made the patient feel better. Historical reports, such as one from 1916, note difficulty associated with eradication of Blastocystis from patients, describing it as "an infection that is hard to get rid of."
A 1999 in vitro study from Pakistan found 40% of isolates are resistant to common antiprotozoal drugs. A study of isolates from patients diagnosed with IBS found 40% of isolates resistant to metronidazole and 32% resistant to furazolidone. Drugs reported in studies to be effective in eradicating Blastocystis infection have included metronidazole, trimethoprim, TMP-SMX (only trimethoprim is active with sulphamethoxazole demonstrating no activity), tetracycline, doxycycline, nitazoxanide, pentamidine, paromomycin and iodoquinol. Iodoquinol has been found to be less effective in practice than in-vitro. Miconazole and quinacrine have been reported as effective agents against Blastocystis growth in-vitro. Rifaximin, and albendazole have shown promise as has ivermectin which demonstrated high effectiveness against blastocystis hominis isolates in an in vitro study. There is also evidence that the probiotic yeast Saccharomyces boulardii, and the plant mallotus oppositifolius may be effective against Blastocystis infections.
Physicians have described the successful use of a variety of discontinued antiprotozoals in treatment of Blastocystis infection. Emetine was reported as successful in cases in early 20th century with British soldiers who contracted Blastocystis infection while serving in Egypt. In vitro testing showed emetine was more effective than metronidazole or furazolidone. Emetine is available in the United States through special arrangement with the Center for Disease Control. Clioquinol (Entero-vioform) was noted as successful in treatment of Blastocystis infection but removed from the market following an adverse event in Japan. Stovarsol and Narsenol, two arsenic-based antiprotozoals, were reported to be effective against the infection. Carbarsone was available as an anti-infective compound in the United States as late as 1991, and was suggested as a possible treatment. The reduction in the availability of antiprotozoal drugs has been noted as a complicating factor in treatment of other protozoal infections. For example, in Australia, production of diloxanide furoate ended in 2003, paromomycin is available under special access provisions, and the availability of iodoquinol is limited.
Epidemiology
Like other protozoal infections, the prevalence of Blastocystis infection varies depending on the area investigated and the population selected. A number of different species groups of Blastocystis infect humans, with some being reported to cause disease while others do not. To date surveys have not distinguished between different types of Blastocystis in humans so the significance of findings may be difficult to evaluate. Developing countries have been reported to have higher incidences, however recent studies suggest that symptomatic infection with Blastocystis may be prevalent in certain industrialized countries as well.
Other animals
Experimental infection in immunocompetent and immunocompromised mice has produced intestinal inflammation, altered bowel habits, lethargy and death. Chronic diarrhea has been reported in non-human higher primates.
Research
While many enteric protists are the subject of research, Blastocystis is unusual in that basic questions concerning how it should be diagnosed and treated and how it causes disease remain unsettled. The following groups have ongoing research programs directed at these questions: