
ICD-9-CM 367.2 DiseasesDB 29648 | ICD-10 H52.2 OMIM 603047 MedlinePlus 001015 | |
 | ||
Astigmatism is a type of refractive error in which the eye does not focus light evenly on the retina. This results in distorted or blurred vision at all distances. Other symptoms can include eyestrain, headaches, and trouble driving at night. If it occurs early in life it can result in amblyopia.
Contents
- Signs and symptoms
- Axis of the principal meridian
- Focus of the principal meridian
- Throughout the eye
- Diagnosis
- Treatment
- Epidemiology
- History
- References
The cause of astigmatism is unclear. It is believed to be partly related to genetic factors. The underlying mechanism involves an irregular curvature of the cornea or abnormalities in the lens of the eye. Diagnosis is by an eye exam.
Three options exist for the treatment: glasses, contact lenses, and surgery. Glasses are the simplest. Contact lenses can provide a wider field of vision. Refractive surgery permanently changes the shape of the eye.
In Europe and Asia astigmatism affects between 30 and 60% of adults. People of all ages can be affected. Astigmatism was first reported by Thomas Young in the early 1800s.
Signs and symptoms
Although astigmatism may be asymptomatic, higher degrees of astigmatism may cause symptoms such as blurry vision, squinting, eye strain, fatigue, or headaches. Some research has pointed to the link between astigmatism and higher prevalence of migraine headaches.
Axis of the principal meridian
In with-the-rule astigmatism, a minus cylinder is placed on the horizontal axis to correct the refractive error (or a plus cylinder in the vertical axis). Adding a minus cylinder in the horizontal axis makes the horizontal axis "steeper" (or better: makes the vertical axis "less steep") which makes both axes equally "steep". In against-the-rule astigmatism, a plus cylinder is added in the horizontal axis (or a minus cylinder in the vertical axis).
Axis is always recorded as an angle in degrees, between 0 and 180 degrees in a counter-clockwise direction. Both 0 and 180 degrees lie on a horizontal line at the level of the center of the pupil, and as seen by an observer, 0 lies on the right of both the eyes.
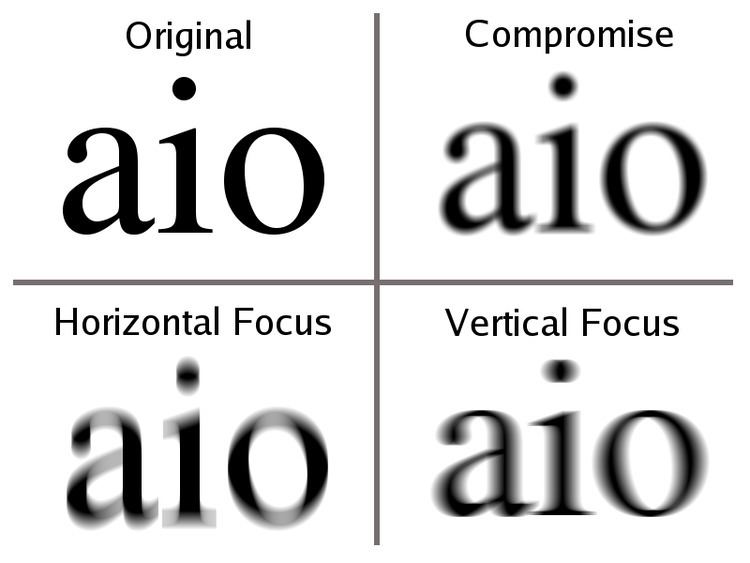
Focus of the principal meridian
With accommodation relaxed:
Throughout the eye
Astigmatism, whether it is regular or irregular, is caused by some combination of external (corneal surface) and internal (posterior corneal surface, human lens, fluids, retina, and eye-brain interface) optical properties. In some people, the external optics may have the greater influence, and in other people, the internal optics may predominate. Importantly, the axes and magnitudes of external and internal astigmatism do not necessarily coincide, but it is the combination of the two that by definition determines the overall optics of the eye. The overall optics of the eye are typically expressed by a person's refraction; the contribution of the external (anterior corneal) astigmatism is measured through the use of techniques such as keratometry and corneal topography. One method analyzes vectors for planning refractive surgery such that the surgery is apportioned optimally between both the refractive and topographic components.
Diagnosis
A number of tests are used during eye examinations to determine the presence of astigmatism and to quantify its amount and axis. A Snellen chart or other eye charts may initially reveal reduced visual acuity. A keratometer may be used to measure the curvature of the steepest and flattest meridians in the cornea's front surface. Corneal topography may also be used to obtain a more accurate representation of the cornea's shape. An autorefractor or retinoscopy may provide an objective estimate of the eye's refractive error and the use of Jackson cross cylinders in a phoropter or trial frame may be used to subjectively refine those measurements. An alternative technique with the phoropter requires the use of a "clock dial" or "sunburst" chart to determine the astigmatic axis and power. A keratometer may also be used to estimate astigmatism by finding the difference in power between the two primary meridians of the cornea. Javal's rule can then be used to compute the estimate of astigmatism.
A method of astigmatism analysis by Alpins may be used to determine both how much surgical change of the cornea is needed and after surgery to determine how close treatment was to the goal.
Another rarely used refraction technique involves the use of a stenopaic slit (a thin slit aperture) where the refraction is determined in specific meridians – this technique is particularly useful in cases where the patient has a high degree of astigmatism or in refracting patients with irregular astigmatism.
There are three primary types of astigmatism: myopic astigmatism, hyperopic astigmatism, and mixed astigmatism.
Treatment
Astigmatism may be corrected with eyeglasses, contact lenses, or refractive surgery. Various considerations involving eye health, refractive status, and lifestyle determine whether one option may be better than another. In those with keratoconus, certain contact lenses often enable patients to achieve better visual acuity than eyeglasses. Once only available in a rigid, gas-permeable form, toric lenses are now available also as soft lenses.
Laser eye surgery (LASIK and PRK) is successful in treating astigmatism.
Epidemiology
According to an American study nearly three in 10 children (28.4%) between the ages of five and 17 have astigmatism. A recent Brazilian study found that 34% of the students in one city were astigmatic. Regarding the prevalence in adults, a recent study in Bangladesh found that nearly 1 in 3 (32.4%) of those over the age of 30 had astigmatism.
A Polish study published in 2005 revealed "with-the-rule astigmatism" may lead to the onset of myopia.
A number of studies have found the prevalence of astigmatism increases with age.
History
As a student, Thomas Young discovered that he had problems with one eye in 1793. In the following years he did research on his vision problems. He presented his findings in a Bakerian Lecture in 1801.
Independent from Young, George Biddell Airy discovered the phoneme of astigmatism on his own eye. Airy presented his observations on his own eye in February 1825 at the Cambridge Philosophical Society. Airy produced lenses to correct his vision problems by 1825, while other sources put this into 1827 when Airy obtained cylindrical lenses from an optician from Ipswich. The name for the condition was not given by Airy, but from William Whewell.
By the 1860s astigmatism was a well established concept in ophthalmology, and chapters in books described the discovery of astigmatism.