
 | ||
Vitamin A deficiency (VAD) or hypovitaminosis A is a lack of vitamin A in blood and tissues. It is common in poorer countries but rarely seen in more developed countries. Nyctalopia (night blindness) is one of the first signs of VAD. Xerophthalmia, keratomalacia, and complete blindness can also occur since Vitamin A has a major role in phototransduction.
Contents
Vitamin A deficiency is the leading cause of preventable childhood blindness and is critical to achieving Millennium Development Goal 4 to reduce child mortality. Approximately 250,000 to 500,000 malnourished children in the developing world go blind each year from a deficiency of vitamin A, approximately half of whom die within a year of becoming blind. The United Nations Special Session on Children in 2002 set a goal of the elimination of VAD by 2010.
The prevalence of night blindness due to VAD is also high among pregnant women in many developing countries. VAD also contributes to maternal mortality and other poor outcomes in pregnancy and lactation.
VAD also diminishes the ability to fight infections. In countries where children are not immunized, infectious diseases like measles have higher fatality rates. As elucidated by Alfred Sommer, even mild, subclinical deficiency can also be a problem, as it may increase children's risk of developing respiratory and diarrheal infections, decrease growth rate, slow bone development, and decrease likelihood of survival from serious illness.
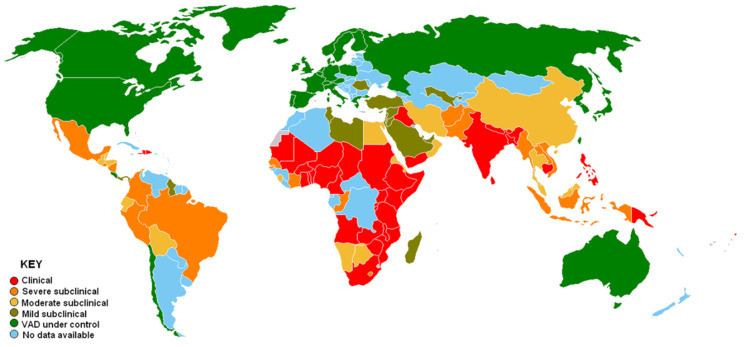
VAD is estimated to affect approximately one third of children under the age of five around the world. It is estimated to claim the lives of 670,000 children under five annually. Approximately 250,000–500,000 children in developing countries become blind each year owing to VAD, with the highest prevalence in Southeast Asia and Africa. According to the World Health Organization (WHO), VAD is under control in the United States, but, in developing countries, VAD is a significant concern. Globally, 65% of all children aged 6 to 59 months received two doses of vitamin A in 2013, fully protecting them against VAD (80% in the least developed countries).
Signs and symptoms
The common cause of blindness in developing countries is VAD. The World Health Organization (WHO) estimates 13.8 million children to have some degree of visual loss related to VAD. Night blindness and its worsened condition, xerophthalmia, are markers of VAD, as it can also lead to impaired immune function, cancer, and birth defects. Collections of keratin in the conjunctiva, known as Bitot's spots, are also seen. Imtiaz's sign is the earliest ocular sign of VAD. Conjunctival epithelial defects occur around lateral aspect of the limbus in subclinical stage of VAD. These conjunctival epithelial defects are not even visible on a biomicroscope, but they take up black stain and become readily visible after instillation of kajal (surma); this is called "Imtiaz's sign".
Night blindness is the difficulty for the eyes to adjust to dim light. Affected individuals are unable to distinguish images in low levels of illumination. People with night blindness have poor vision in the darkness, but see normally when adequate light is present.
VAD affects vision by inhibiting the production of rhodopsin, the eye pigment responsible for sensing low light situations. Rhodopsin is found in the retina and is composed of retinal (an active form of vitamin A) and opsin (a protein). Because the body cannot create retinal in sufficient amounts, a diet low in vitamin A will lead to a decreased amount of rhodopsin in the eye, as there is inadequate retinal to bind with opsin. Night blindness results.
Night blindness caused by VAD has been associated with the loss of goblet cells in the conjunctiva, a membrane covering the outer surface of the eye. Goblet cells are responsible for secretion of mucus, and their absence results in xerophthalmia, a condition where the eyes fail to produce tears. Dead epithelial and microbial cells accumulate on the conjunctiva and form debris that can lead to infection and possibly blindness.
Decreasing night blindness requires the improvement of vitamin A status in at-risk populations. Supplements and fortification of food have been shown to be effective interventions. Supplement treatment for night blindness includes high doses of vitamin A (200,000 IU) in the form of retinyl palmitate to be taken by mouth, which is administered two to four times a year. Intramuscular injections are poorly absorbed and are ineffective in delivering sufficient bio-available vitamin A. Fortification of food with vitamin A is costly, but can be done in wheat, sugar, and milk. Households may circumvent expensive fortified food by altering dietary habits. Consumption of yellow-orange fruits and vegetables rich in carotenoids, specifically beta-carotene, provides pro-vitamin A precursors that can prevent VAD related night blindness. However, the conversion of carotene to retinol varies from person to person and bioavailability of carotene in food varies.
The richest animal sources of Vitamin A (retinol) are livers like beef liver (one ounce provides around 8,000 IUs ) and Cod Liver Oil (one teaspoon provides around 4,500 IUs ).
Vitamin A deficiency is one of several hypovitaminoses implicated in follicular hyperkeratosis.
Causes
The major cause is roughage which include few animal sources of pre-formed vitamin A. In addition to dietary problems, there are other causes of VAD. Iron deficiency can affect vitamin A uptake. Excess alcohol consumption can deplete vitamin A, and a stressed liver may be more susceptible to vitamin A toxicity. People who consume large amounts of alcohol should seek medical advice before taking vitamin A supplements. In general, people should also seek medical advice before taking vitamin A supplements if they have any condition associated with fat malabsorption such as pancreatitis, cystic fibrosis, tropical sprue and biliary obstruction. Other causes of Vitamin A deficiency are inadequate intake, fat malabsorption, or liver disorders. Deficiency impairs immunity and hematopoiesis and causes rashes and typical ocular effects (eg, xerophthalmia, night blindness).
Infection rates
Along with poor diet there is a large amount of infection and disease present in many developing communities. Infection is very draining on vitamin A reserves and this vitamin A deficit leaves the individual more susceptible to infection (Combs, 1991); increased documentation of xerophthalmia has been seen after an outbreak of measles and the varying stages of xerophthalmia become a good reference point for the extent of deficiency (with mortality increasing with severity of the eye disease). In a longitudinal study of preschool Indonesian children it was found that susceptibility to disease increased nine times when severe VAD was present (Dole 2009).
The reason for the increased infection rate in vitamin A deficient populations is due to the T-killer cells which require retinoids to proliferate correctly (Athanassiades1981). Retinoic acid binds the promoter region of specific genes and so activates the transcription process and therefore cell replication (Baron 1981). A vitamin A deficient diet will have a very limited surplus of retinol and so cell proliferation and replication will be suppressed, contributing to a reduced number of T-cells and lymphocytes. Suppression of these will result in a lack of immune reaction if pathogens become present in the body and consequently a greater susceptibility to incubation of disease.
VAD and infections aggravate each other and therefore with infection the vitamin A levels are depleted which in turn reduces intestinal absorption of vitamin A (WHO 1982). Very often seen with VAD is protein energy malnutrition (PEM). With PEM the synthesis of retinol binding protein (RBP) is decreased, consequently the uptake of retinol is reduced (Combs, 1991). This leads to an inability to utilise any vitamin A present as the RBP is absent and so the retinol cannot be transported to the liver maximising the VAD (Ikekpeazu 2010).
Treatment
Treatment of VAD can be undertaken with both oral and injectable forms, generally as vitamin A palmitate.
Global initiatives
Global efforts to support national governments in addressing VAD are led by the Global Alliance for Vitamin A (GAVA), which is an informal partnership between A2Z, the Canadian International Development Agency, Helen Keller International, Micronutrient Initiative, UNICEF, USAID, and the World Bank. Joint GAVA activity is coordinated by the Micronutrient Initiative.
Vitamin Angels has committed itself to eradicating childhood blindness due to VAD on the planet by the year 2020. Operation 20/20 was launched in 2007 and will cover 18 countries. The program gives children two high-dose vitamin A and anti-parasitic supplements (twice a year for four years), which provides children with enough of the nutrient during their most vulnerable years in order to prevent them from going blind and suffering from other life-threatening diseases caused by VAD.
About 75 per cent of the vitamin A required for supplementation activity by developing countries is supplied by the Micronutrient Initiative with support from the Canadian International Development Agency.
An estimated 1.25 million deaths due to VAD have been averted in 40 countries since 1998.
In 2008 it was estimated that an annual investment of US$60 million in vitamin A and zinc supplementation combined would yield benefits of more than US$1 billion per year, with every dollar spent generating benefits of more than US$17. These combined interventions were ranked by the Copenhagen Consensus 2008 as the world’s best development investment.