
Specialty urology ICD-9-CM 598 MedlinePlus 001271 | ICD-10 N35 DiseasesDB 13562 eMedicine med/3075 | |
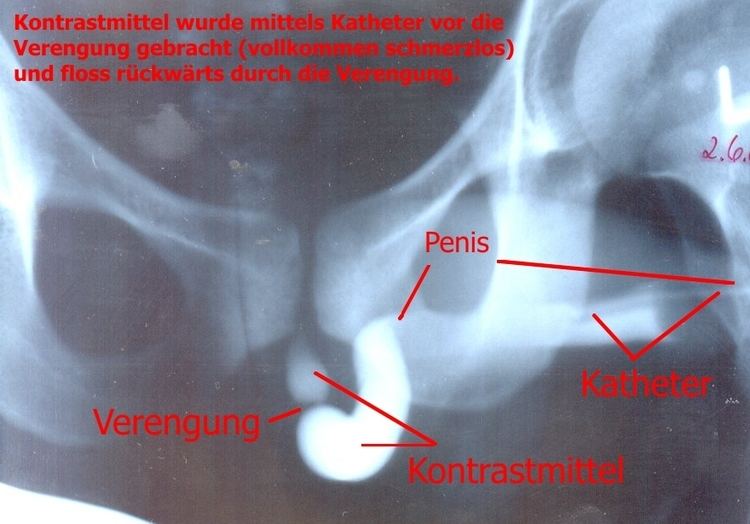 | ||
A urethral stricture is a narrowing of the urethra caused by injury, instrumentation, infection and certain non-infectious forms of urethritis.
Contents
Signs and symptoms
The hallmark sign of urethral stricture is a weak urinary stream. Other symptoms include:
Some patients with severe urethral strictures are completely unable to urinate. This is referred to as acute urinary retention, and is a medical emergency. Hydronephrosis and renal failure may also occur.
Causes
Urethral strictures most commonly result from injury, urethral instrumentation, infection, non-infectious inflammatory conditions of the urethra, and after prior hypospadias surgery. Less common causes include congenital urethral strictures and those resulting from malignancy.
Urethral strictures after blunt trauma can generally be divided into two sub-types.
Other specific causes of urethral stricture include
Diagnosis
Dilation and other endoscopic approaches
Urethral dilation and other endoscopic approaches such as direct vision internal urethrotomy (DVIU), laser urethrotomy, and self intermittent dilation are the most commonly used treatments for urethral stricture. However, these approaches are associated with low success rates and may worsen the stricture, making future attempts to surgically repair the urethra more difficult.
A Cochrane review found that performing intermittent self-dilatation may confer a reduced risk of recurrent urethral stricture after endoscopic treatment, but the evidence is weak.
Urethroplasty
Urethroplasty refers to any open reconstruction of the urethra. Success rates range from 85% to 95% and depend on a variety of clinical factors, such as stricture as the cause, length, location, and caliber. Urethroplasty can be performed safely on men of all ages.
In the posterior urethra, anastomotic urethroplasty (with or without preservation of bulbar arteries) is typically performed after removing scar tissue.
In the bulbar urethra, the most common types of urethroplasty are anastomotic (with or without preservation of corpus spongiosum and bulbar arteries) and substitution with buccal mucosa graft, full-thickness skin graft, or split thickness skin graft. These are nearly always done in a single setting (or stage).
In the penile urethra, anastomotic urethroplasties are rare because they can lead to chordee (penile curvature due to a shortened urethra). Instead, most penile urethroplasties are substitution procedures utilizing buccal mucosa graft, full-thickness skin graft, or split thickness skin graft. These can be done in one or more setting, depending on stricture location, severity, cause and patient or surgeon preference.
Urethral stent
A permanent urethral stent was approved for use in men with bulbar urethral strictures in 1996, but was recently removed from the market.
A temporary thermoexpandable urethral stent (Memotherm) is available in Europe, but is not currently approved for use in the United States.
Emergency treatment
When in acute urinary retention, treatment of the urethral stricture or diversion is an emergency. Options include:
Ongoing care
Following urethroplasty, patients should be monitored for a minimum of 1 year, since the vast majority of recurrences occur within 1 year.
Because of the high rate of recurrence following dilation and other endoscopic approaches, the provider must maintain a high index of suspicion for recurrence when the patient presents with obstructive voiding symptoms or urinary tract infection.
Research
The use of bioengineered urethral tissue is promising, but still in the early stages. The Wake Forest Institute of Regenerative Medicine has pioneered the first bioengineered human urethra, and in 2006 implanted urethral tissue grown on bioabsorbable scaffolding (approximating the size and shape of the affected areas) in five young (human) males who suffered from congenital defects, physical trauma, or an unspecified disorder necessitating urethral reconstruction. As of March, 2011, all five recipients report the transplants have functioned well.