
Passengers 181 Fatalities 10 Number of deaths 10 Injuries (nonfatal) 24 Survivor 179 | Crew 8 Survivors 179 Date 28 December 1978 | |
 | ||
Summary Fuel exhaustion due to pilot error (lack of situational awareness) and maintenance error with landing gear Similar Southern Airways Flight 242, American Airlines Flight 191, 1956 Grand Canyon, Air France Flight 296, United Airlines Flight 232 | ||
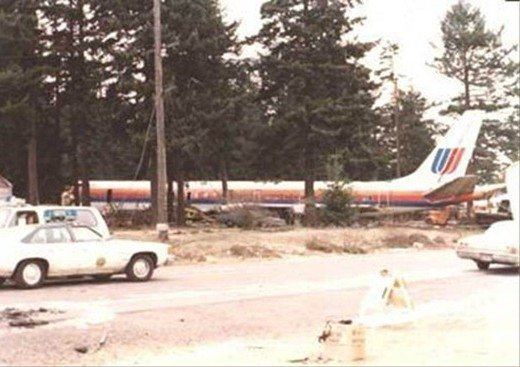
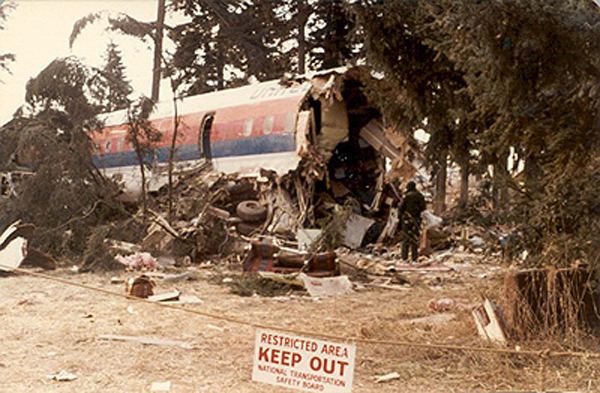
United Airlines Flight 173 was a scheduled flight from John F. Kennedy International Airport in New York City, New York to Portland International Airport in Portland, Oregon, with a scheduled stop in Denver, Colorado. On December 28, 1978, the aircraft flying this route ran out of fuel and crashed in a suburban Portland neighborhood near NE 158th Avenue and East Burnside Street.
Contents
- United airlines flight 173 1978
- Flight
- Crash investigation and report
- Aftermath
- Similar accidents
- References

United airlines flight 173 1978
Flight

Flight 173 was piloted by an experienced cockpit crew, consisting of Captain Malburn McBroom (52), First Officer Roderick Beebe (45), and Flight Engineer Forrest Mendenhall (41). McBroom had been with United Airlines for 27 years; he was one of the airline's most senior pilots with more than 27,600 hours of flight time, of which about 5,500 hours had been as a DC-8 captain. Beebe had been with the airline for 13 years and had logged more than 5,200 flight hours. Mendenhall had accrued close to 3,900 flight hours and had been with the airline for 11 years. The first officer and flight engineer had over 2,500 hours of flying experience between them in the DC-8.

Flight 173 departed from Denver about 14:47 with 189 people on board. The estimated time en route was 2 hours and 26 minutes. The planned arrival time in Portland was 17:13. According to the automatic flight plan and monitoring system, the total amount of fuel required for the flight to Portland was 31,900 lbs. There was 46,700 lbs. of fuel on board the aircraft when it departed the gate in Denver.
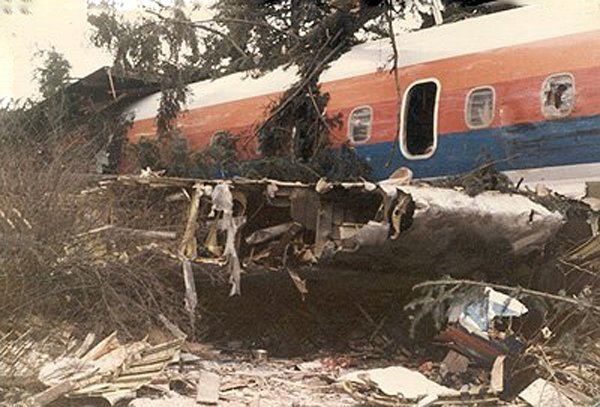
As the landing gear was being lowered on approach to Portland International Airport, the crew felt an abnormal vibration and yaw of the aircraft as well as a lack of an indicator light showing the gear was lowered unsuccessfully. The crew requested a holding pattern to diagnose the problem, and for approximately the next hour the crew worked to identify the status of the landing gear and prepare for a potential emergency landing. During this time, none of the three cockpit flight crew effectively monitored the fuel levels, which was exacerbated by the fact that the gear was down with the flaps at 15 degrees during the entire hour-long holding maneuver, significantly increasing fuel burn rate. As the crew prepared for a final approach for an emergency landing into Portland, they lost the number one and number two engines to flameout, at which point a mayday was declared. This was the last radio transmission from Flight 173 to Air Traffic Control. The plane crashed into a wooded section of a populated area of suburban Portland about 6 nautical miles southeast of the airport.
Of the crew members, two were killed, Flight Engineer Mendenhall and Flight Attendant Joan Wheeler, two sustained injuries classified by the National Transportation Safety Board (NTSB) as "serious", and four sustained injuries classified as "minor/none." Eight passengers died, and 21 had serious injuries.

The 304th Aerospace Rescue and Recovery Squadron of the Air Force Reserve, based at Portland International Airport, was conducting routine training flights in the area that evening. Airborne aircraft from this unit (HH-1H Huey helicopters) were immediately diverted to the crash scene and proceeded to transport many of the survivors to local hospitals.
Crash investigation and report
The NTSB investigation revealed that when the landing gear was lowered, a loud thump was heard. That unusual sound was accompanied by abnormal vibration and yaw of the aircraft. The right main landing gear retract cylinder assembly had failed due to corrosion, and that allowed the right gear to free fall. Although it was down and locked, the rapid and abnormal free fall of the gear damaged a microswitch so severely that it failed to complete the circuit to the cockpit green light that tells the pilots that gear is down and locked. Those unusual indications (loud noise, vibration, yaw, and no green light) led the captain to abort the landing, so that they would have time to diagnose the problem and prepare the passengers for an emergency landing. While the decision to abort the landing was prudent, the accident occurred because the flight crew became so absorbed with diagnosing the problem that they failed to monitor their fuel state and calculate a time when they needed to return to land or risk fuel exhaustion.
"The Safety Board believes that this accident exemplifies a recurring problem—a breakdown in cockpit management and teamwork during a situation involving malfunctions of aircraft systems in flight… Therefore, the Safety Board can only conclude that the flightcrew failed to relate the fuel remaining and the rate of fuel flow to the time and distance from the airport, because their attention was directed almost entirely toward diagnosing the landing gear problem."
The NTSB determined the following probable cause:
The failure of the captain to monitor properly the aircraft's fuel state and to properly respond to the low fuel state and the crewmember's advisories regarding fuel state. This resulted in fuel exhaustion to all engines. His inattention resulted from preoccupation with a landing gear malfunction and preparations for a possible landing emergency.
The NTSB also determined the following contributing factor:
The failure of the other two flight crewmembers either to fully comprehend the criticality of the fuel state or to successfully communicate their concern to the captain.
The fuel situation was known to be on the minds of the pilot and crew to some degree. Transcripts of cockpit recordings confirm this. Media reports at the time suggested that there was a not widely known problem with fuel state gauges on that model aircraft.. The problem was not widely known in part because commercial aircraft are expected to fly with not less than a 45-minute reserve of fuel at all times. The gauge problem is addressed, though obliquely, in one of the safety board's recommendations:
Issue an Operations Alert Bulletin to have FAA inspectors assure that crew training stresses differences in fuel-quantity measuring instruments and that crews flying with the new system are made aware of the possibility of misinterpretation of gauge readings. (Class II--Priority Action) (A-79-32)
While the totalizer fuel gauge issue might have contributed to the crew's confusion toward the end of the flight, the NTSB report emphasized that the captain should never have allowed such a situation to develop in the first place. The NTSB made the following recommendation to specifically address that concern:
Issue an operations bulletin to all air carrier operations inspectors directing them to urge their assigned operators to ensure that their flightcrews are indoctrinated in principles of flightdeck resource management, with particular emphasis on the merits of participative management for captains and assertiveness training for other cockpit crewmembers. (Class II, Priority Action) (X-79-17)
Aftermath
This last NTSB recommendation following the incident, addressing flightdeck resource management problems, was the genesis for major changes in the way airline crewmembers were trained. This new type of training addressed behavioral management challenges such as poor crew coordination, loss of situational awareness, and judgment errors frequently observed in aviation accidents. It is credited with launching the crew resource management (CRM) revolution in airline training. Within weeks of the NTSB recommendation, NASA held a conference to bring government and industry experts together to examine the potential merits of this training.
United Airlines instituted the industry's first crew resource management (CRM) for pilots in 1981. The CRM program is now used throughout the world, prompting some to call the United 173 accident one of the most important in aviation history. The NTSB Air Safety Investigator who wrote the CRM recommendation was aviation psychologist Alan Diehl.
Assigned to investigate this accident, Diehl realized it was similar to several other major airline accidents including United Airlines Flight 2860, which occurred a little over a year before Flight 173 and under similar circumstances; Eastern Air Lines Flight 401; and the Tenerife airport disaster. Diehl was familiar with the research being conducted at NASA’s Ames Research Center and believed these training concepts could reduce the likelihood of human error.
Held responsible for the accident, Captain McBroom lost his pilot's license and retired from United Airlines shortly afterwards. He spent his remaining years battling numerous health issues related to injuries sustained in the crash as well as lung and prostate cancer. Family members and passengers who spoke to McBroom at a 1998 reunion of crash survivors reported he was "a broken man" plagued by guilt over his role in the accident. He died on October 9, 2004 at age 77.
Similar accidents
Other aircraft accidents involving faulty landing gear indicator lights include:
An almost identical situation happened in 1963 with Aeroflot Tu-124, which ditched into the Neva River due to fuel exhaustion after circling for two hours in the vicinity of Pulkovo airport, while the crew tried to troubleshoot landing gear problems. Everyone on board survived.
Scandinavian Airlines System Flight 933, on January 13, 1969, crashed into the ocean during an approach to Los Angeles International Airport also using a DC-8. The green light for the nose gear failed to illuminate after the landing gear was lowered. The SAS cockpit crew became so occupied with attempting to diagnose the lack of a nose gear green light that they allowed their rate of descent to increase, until their DC-8-62 crashed into the ocean, well short of the runway.
Eastern Air Lines Flight 401 crashed while circling around the airport at Miami, on December 29, 1972, The Eastern crew became preoccupied with the nose gear indicator light problem and accidentally disconnected the autopilot, causing the aircraft to make a slow descent and crash into the Everglades. Further investigation revealed that the nose gear was down and locked.
LOT Flight 7 on March 14, 1980
United Airlines Flight 2860 on December 17, 1977
Other incidents involving a holding pattern leading to fuel starvation:
Avianca Flight 52, on January 25, 1990, crashed in New York, after being put in three holding patterns over the course of the flight, leading to a crash in New York City from Fuel starvation