
Specialty medical genetics ICD-9-CM 530.84, 750.3 eMedicine med/3416 | ICD-10 J95.0, Q39.1-Q39.2 DiseasesDB 30034 MeSH D014138 | |
 | ||
A tracheoesophageal fistula (TEF, or TOF; see spelling differences) is an abnormal connection (fistula) between the esophagus and the trachea. TEF is a common congenital abnormality, but when occurring late in life is usually the sequela of surgical procedures such as a laryngectomy.
Contents
Causes
Congenital TEF can arise due to failed fusion of the tracheoesophageal ridges after the fourth week of embryological development.
A fistula, from the Latin meaning ‘a pipe,’ is an abnormal connection running either between two tubes or between a tube and a surface. In tracheo-esophageal fistula it runs between the trachea and the esophagus. This connection may or may not have a central cavity; if it does, then food within the esophagus may pass into the trachea (and on to the lungs) or alternatively, air in the trachea may cross into the esophagus.
TEF can also occur due to pressure necrosis by a tracheostomy tube in apposition to a nasogastric tube (NGT).
Associations
Neonates with TEF or esophageal atresia are unable to feed properly. Once diagnosed, prompt surgery is required to allow the food intake. Some children do experience problems following TEF surgery; they can develop dysphagia and thoracic problems. Children with TEF can also be born with other abnormalities, most commonly those described in VACTERL association - a group of anomalies which often occur together, including heart, kidney and limb deformities. 6% of babies with TEF also have a laryngeal cleft.
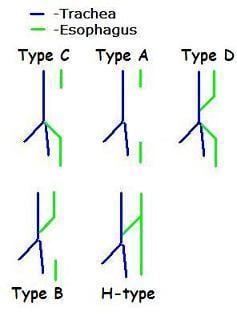
Classification
Fistulae between the trachea and esophagus in the newborn can be of diverse morphology and anatomical location; however, various pediatric surgical publications have attempted a classification system based on the below specified types.
Not all types include both esophageal agenesis and tracheoesophageal fistula, but the most common types do.
The letter codes are usually associated with the system used by Gross, while number codes are usually associated with Vogt.
An additional type, "blind upper segment only" has been described, but this type is not usually included in most classifications.
(For the purposes of this discussion, proximal esophagus indicates normal esophageal tissue arising normally from the pharynx, and distal esophagus indicates normal esophageal tissue emptying into the proximal stomach.)
Clinical presentation
Tracheoesophageal fistula is suggested in a newborn by copious salivation associated with choking, coughing, vomiting, and cyanosis coincident with the onset of feeding. Esophageal atresia and the subsequent inability to swallow typically cause polyhydramnios in utero. Rarely it may present in an adult.
Treatment
It is surgically corrected, with resection of any fistula and anastomosis of any discontinuous segments. Surgical repair is associated with complications, including