
 | ||
A tourniquet is a constricting or compressing device, specifically a bandage, used to control venous and arterial circulation to an extremity for a period of time. Pressure is applied circumferentially upon the skin and underlying tissues of a limb; this pressure is transferred to the walls of vessels, causing them to become temporarily occluded. It is generally used as a tool for a medical professional in applications such as cannulation or to stem the flow of traumatic bleeding, especially by military medics. The tourniquet is usually applied when the patient is in a life-threatening state as a result of continuous bleeding.
Contents
- History
- Types
- Surgical tourniquets
- Pneumatic Tourniquets
- Contoured cuffs
- Limb occlusion pressure
- Limb protection
- Silicone Ring Tourniquets
- Complications
- Emergency tourniquets
- Current technology
- Mass Casualty Tourniquet
- Silicone Ring Auto Transfusion Tourniquet
- CombatSelf Applied Tourniquet
- Automatic systems
- Contoured and wide cuffs
- Integrated tourniquet cuff testing
- References
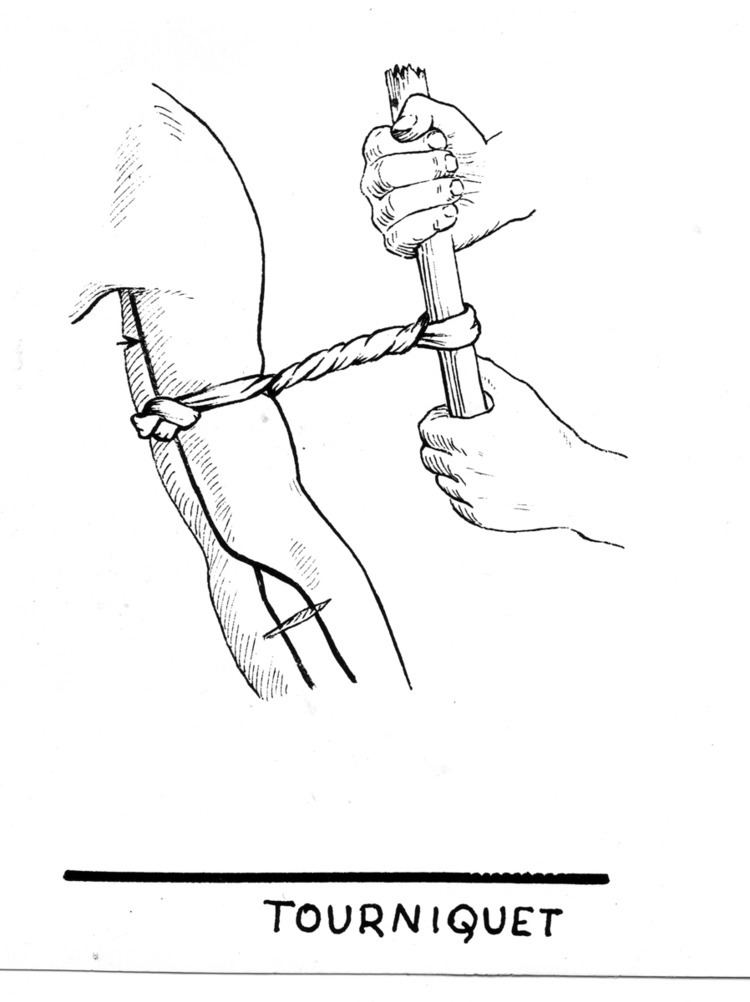
A primitive tourniquet can be made from a stick and a rope (or leather belt). The rope is made into a loop that fits over the damaged limb and the stick is inserted through the loop. The loop is tightened by twisting the stick. This primitive device stems the flow of blood but side-effects such as tissue damage and nerve damage may occur. In modern medicine, pre-assembled devices have been developed. They avoid side-effects of the traditional rope-and-stick tourniquets and can be faster or easier to apply. Some modern tourniquets, such as the Combat Application Tourniquet or the SOF Tourniquet can be applied with one hand by the injured person himself. However, it does require some practice to ensure it is applied correctly and quickly.
History
During Alexander the Great’s military campaigns in the fourth century BC, tourniquets were used to stanch the bleeding of wounded soldiers. Romans used them to control bleeding, especially during amputations. These tourniquets were narrow straps made of bronze, using only leather for comfort.
In 1718, French surgeon Jean Louis Petit developed a screw device for occluding blood flow in surgical sites. Before this invention, the tourniquet was a simple garrot, tightened by twisting a rod (thus its name tourniquet, from tourner = to turn).
In 1785 Sir Gilbert Blane advocated that, in battle, each Royal Navy sailor should carry a tourniquet:
“It frequently happens that men bleed to death before assistance can be procured, or lose so much blood as not to be able to go through an operation. In order to prevent this, it has been proposed, and on some occasions practised, to make each man carry about him a garter, or piece of rope yarn, in order to bind up a limb in case of profuse bleeding. If it be objected, that this, from its solemnity may be apt to intimidate common men, officers at least should make use of some precaution, especially as many of them, and those of the highest rank, are stationed on the quarter deck, which is one of the most exposed situations, and far removed from the cockpit, where the surgeon and his assistants are placed. This was the cause of the death of my friend Captain Bayne, of the Alfred, who having had his knee so shattered with round shot that it was necessary to amputate the limb, expired under the operation, in consequence of the weakness induced by loss of blood in carrying him so far. As the Admiral on these occasions allowed me the honour of being at his side, I carried in my pocket several tourniquets of a simple construction, in case that accidents to any person on the quarter deck should have required their use.”
Joseph Lister is credited for being the first to use a tourniquet device to create a bloodless surgical field in 1864. He also recommended exsanguinations prior to tourniquet application by limb elevation. In 1873, Friedrich von Esmarch developed a rubber bandage that would both control bleeding and exsanguinate. This device is known as Esmarch's bandage for surgical haemostasis or Eschmarch's Tourniquet. At the time this device was superior to Petit’s device as there were no screws to loosen or cloth to tear. In 1881, Richard von Volkmann showed that limb paralysis can occur from the use of the Esmarch tourniquet.
In 1904, Harvey Cushing created a pneumatic tourniquet. This type of tourniquet compressed the underlying blood vessels using a compressed gas source to inflate a cylindrical bladder. This was superior to the Esmarch tourniquet in two ways: (1) the tourniquet could be applied and removed quickly; and (2) this method of limb occlusion decreased the incidence of nerve paralysis.
August Bier used two tourniquets for administering segmental anesthesia in 1908. In this procedure circulation is isolated in a limb and the limb is then infused intravenously. In 1963 Hamilton E. Holmes reintroduced Bier’s method as a single tourniquet technique. Today, the two-tourniquet technique is used frequently and is called intravenous regional anesthesia (IVRA). It is also commonly referred to as Bier block, or Bier’s method.
In the early 1980s microprocessor-controlled tourniquets were invented by James McEwen, a biomedical engineer in Vancouver, Canada. The first US patent for an electronic tourniquet system was awarded to Dr. McEwen in 1984 and to date he has been awarded many more US and foreign patents for tourniquet improvements. The use of automatic tourniquet systems has significantly improved tourniquet safety. Modern automatic tourniquets are self-calibrating and self-contained. These new tourniquet devices also provide a variety of safety features that are not possible in older mechanical tourniquets.
In the 2000s, the silicon ring tourniquet, or elastic ring tourniquet, was developed by Dr. Noam Gavriely, a professor of medicine and former emergency physician. The tourniquet consists of an elastic ring made of silicone, stockinet, and pull straps made from ribbon that are used to roll the device onto the limb. The silicone ring tourniquet exsanguinates the blood from the limb while the device is being rolled on, and then occludes the limb once the desired occlusion location is reached. Unlike the historical mechanical tourniquets, the device reduces the risk of nerve paralysis. The surgical tourniquet version of the device is completely sterile, and provides improved surgical accessibility due to its narrow profile that results in a larger surgical field. It has been found to be a safe alternative method for most orthopedic limb procedures, but it does not completely replace the use of contemporary tourniquet devices. More recently the silicone ring tourniquet has been used in the fields of emergency medicine and vascular procedures.
After World War II, the US military reduced use of the tourniquet because the time between application and reaching medical attention was so long that the damage from stopped circulation was worse than that from blood loss. Since the beginning of the 21st century, US authorities have resuscitated its use in both military and non-military situations because treatment delays have been dramatically reduced. The Virginia State Police and police departments in Dallas, Philadelphia and other major cities provide tourniquets and other advanced bandages. In Afghanistan and Iraq, only 2 percent of soldiers with severe bleeding died compared with 7 percent in the Vietnam War, in part because of the combination of tourniquets and rapid access to doctors. In civilian use, emerging practices include transporting tourniquetted patients even before emergency responders arrive and including tourniquets with defibrillators for emergency use.
Types
There are two types of tourniquets: surgical tourniquets and emergency tourniquets. Surgical tourniquets are frequently used in orthopedic surgery while emergency tourniquets are limited to emergency situations to control blood loss.
Surgical tourniquets
Surgical tourniquets prevent blood flow to a limb and enable surgeons to work in a bloodless operative field. This allows surgical procedures to be performed with improved precision, safety and speed. Tourniquets are widely used in orthopedic and plastic surgery, as well as in intravenous regional anesthesia (Bier block anesthesia) where they serve the additional function of preventing local anesthetic in the limb from entering general circulations.
In the early 1980s, microprocessor-controlled pneumatic tourniquets were invented by James McEwen. Automatic tourniquets based on this invention are now standard equipment in operating rooms worldwide, and these systems have significantly improved the safety and convenience of tourniquet use. In the 2000s, a modern mechanical tourniquet called either a silicone ring tourniquet, or elastic ring tourniquet, was invented by Prof. Noam Gavriely. The surgical tourniquet version of the device, and provides improved surgical accessibility due to its narrow profile that results in a larger surgical field. It can be used for most limb procedures, but it does not completely replace the use of contemporary tourniquet devices.
Despite many advances in tourniquet technology, tourniquet-related injuries continue to be of concern. High pressures under a tourniquet cuff can cause nerve, muscle and skin injury. Minimizing tourniquet pressure and reducing tourniquet time help to reduce the risk of tourniquet-related injury.
Pneumatic Tourniquets
Modern pneumatic tourniquets have three basic components: an inflatable cuff, a compressed gas source, and an instrument which automatically monitors and controls cuff pressure. The cuff is secured around the limb proximal to the operative site. Pressure is exerted on the circumference of the limb by means of compressed gas which is introduced into the tourniquet cuff by a microprocessor-controlled source, via connection tubing. When sufficient pressure is exerted, vessels and arteries beneath the cuff become temporarily occluded, preventing blood flow past the cuff. While the cuff is inflated, the tourniquet system automatically monitors and maintains the pressure chosen by the user. Cuff pressure and inflation time are displayed, and an audiovisual alarm alerts the user to alarm conditions, such as a cuff leak.
Contoured cuffs
Studies have shown that tourniquet cuff pressures can be substantially reduced without compromising the quality of surgical field by using wide, contoured cuffs. Wide cuffs also reduce the risk of injury to underlying tissue by dispersing the cuff’s force over a greater surface area. Standard cuffs are relatively narrow in width and are cylindrical in shape. Where there is a significant difference in limb circumference between the distal and proximal edges of the cuff, a contoured cuff with a tapered, conical shape provides a more anatomical fit and maximizes the contact area between cuff and limb. Wide cuffs with an adjustable, variable taper have recently been introduced, permitting one cuff to conform to a variety of limb shapes.
Limb occlusion pressure
Limb occlusion pressure (LOP) is the minimum tourniquet pressure required to occlude blood flow to a specific patient's limb at a specific time, and takes into account a patient’s limb and vessel characteristics, and the type and fit of the cuff. LOP can be determined by gradually increasing tourniquet pressure until distal arterial pulses cease, as indicated by a device sensing blood flow, such as a Doppler stethoscope. Studies have shown that cuff pressure based on LOP measured immediately prior to surgery is generally lower than pressure from commonly used cuffs and is sufficient to maintain a satisfactory surgical field. Traditionally, this method has not been used because it is time consuming and technically demanding. However, a pneumatic tourniquet that uses an automated plethysmographic system to calculate LOP in approximately 30 seconds at the beginning of surgery has recently been developed. This device has similar accuracy to the standard Doppler technique and addresses the practicality of using LOP in the operating room.
Limb protection
For some cuffs, a matching limb protection sleeve is available to help protect soft tissues under the cuff. Without proper protection, underlying soft tissue is prone to damage caused by wrinkling, pinching or shearing. Sleeves are sized according to the cuff width and the patient’s limb circumference. They are intended to fit snugly and extend beyond the edge of the cuff to ensure that there is no direct contact between cuff and skin. Sleeve materials that do not shed loose fibers are chosen to avoid lint becoming trapped in the cuff’s hook and loop fasteners, which reduces their effectiveness.
Silicone Ring Tourniquets
Silicone ring tourniquets, or elastic ring tourniquets, are self-contained mechanical devices that do not require any electricity, wires or tubes. The tourniquet comes in a variety of sizes. To determine the correct product size, the patient's limb circumference at the desired occlusion location should be measured, as well as their blood pressure to determine the best model. Once the correct model is selected, between two sterile medical personnel will be needed to apply the device. It should be noted, unlike with the pneumatic tourniquet, the silicone ring tourniquet should be applied after the drapes have been placed on the patient. This is due to the device being completely sterile. The majority of the devices require a two-man operation (with the exception of the extra large model):
- One person is responsible for holding the patient's limb, the other will place the device on the limb (with the extra-large there are two people needed).
- Application:
- Place the elastic ring tourniquet on the hand/foot. Take care to ensure that all the fingers/toes are enclosed within the device.
- The handles of the tourniquet should be positioned medial-lateral on the upper extremity or posterior-anterior on the lower extremity.
- The person applying the device should start rolling the device while the individual responsible for the limb should hold the limb straight and maintain axial traction.
- Once the desired occlusion location is reached, the straps can be cut off or tied just below the ring.
- A window can be cut or the section of stockinet can be completely removed.
- Once the surgery is completed the device is cut off with a supplied cutting card.
The elastic ring tourniquet follows similar recommendations noted for pneumatic tourniquet use:
- It should not be used on a patient's limb for more than 120 minutes.
- The tourniquet should not be placed on the ulnar/peroneal nerve.
- The silicone ring device cannot be used on patients with blood problems such as DVT, edema, etc.
- A patient suffering from skin lesions or a malignancy should use this type of tourniquet.
Complications
Complications of tourniquet application 1. Tourniquet pain - Characterized by hyperemia, hyperthermia and pain following reperfusion 2. Post-tourniquet syndrome - Manifesting as pain, numbness, paresis, stiffness and pallor 3. Skin changes - Blistering, ischemic necrosis 4. Compartment syndrome 5. Cerebral hypoxia
Emergency tourniquets
Emergency tourniquets are used in emergency bleeding control to prevent severe blood loss from limb trauma. Traditionally, emergency tourniquets are generally used as a last resort, especially in civilian applications, due to the understanding that if all blood flow below the application of an emergency tourniquet is stopped, it would subsequently kill the tissue, leading to eventual loss of the limb below application. More recently, experience in treatment of patients in civilian attacks such as the Boston Marathon bombing, and combat in Iraq and Afghanistan has changed the view of some within the emergency medicine field.
Uncontrolled hemorrhage is the most preventable cause of deaths on both the battlefield and the streets of the United States. Studies show up to 50% of combat fatalities and 39% of civilian trauma fatalities are due to uncontrolled hemorrhage from an extremity. It is possible to die of exsanguination from femoral arterial bleeding in as little as three minutes. Use of tourniquets is widespread in military applications, as they have the potential to save lives during major limb trauma. Analysis has shown that in cases of major limb trauma, there is no apparent link between tourniquet application and morbidity of the limb.
Current technology
In recent years there have been significant advancements in tourniquets. These advancements have vastly improved tourniquet safety.
Mass Casualty Tourniquet
S.T.A.T. Tourniquet is currently the only tourniquet that has an automatic counting timer that requires no batteries and can be applied in 5 seconds by a person with no experience in Mass Casualty Incidents (MCI). S.T.A.T. Tourniquet is designed so multiple tourniquets can be linked together to create a Torso Compression Strap for lacerations or bullet wounds. http://www.emsworld.com/product/12240209/smart-products-llc-stat-tourniquet smarttourniquet.com
Silicone Ring Auto-Transfusion Tourniquet
The silicone ring auto-transfusion tourniquet (SRT/ATT/EED), or Surgical Auto-Transfusion Tourniquet (HemaClear), is a simple to use, self-contained, mechanical tourniquet that consists of a silicone ring, stockinet, and pull straps that results in the limb being exsanguinated and occluded within seconds of application. The tourniquet can be used for limb procedures in the operating room, or in emergency medicine as a means to stabilize a patient until further treatment can be applied.
Limb occlusion pressure
Limb occlusion pressure (LOP) is the minimum tourniquet pressure required to occlude blood flow to a specific patient's limb at a specific time and accounts for a patient’s limb and vessel characteristics, and the type and fit of the cuff. LOP can be determined by gradually increasing tourniquet pressure until distal arterial pulses cease, as indicated by a device sensing blood flow, such as a Doppler stethoscope. Studies have shown that cuff pressure based on LOP measured immediately prior to surgery is generally lower than commonly used cuff pressures and is sufficient to maintain a satisfactory surgical field.
Combat/Self-Applied Tourniquet
The Combat Application Tourniquet (C-A-T) was developed by Composite Resources, Inc. and is used by the U.S. and Coalition military to provide soldiers a small and effective tourniquet in field combat situations, and is also in use by NHS ambulance services, and some UK fire and rescue services. The unit utilizes a windlass with a locking mechanism and can be self-applied. The (C-A-T) has been adopted by military and emergency personnel around the world.
Automatic systems
Automatic tourniquet systems are capable of providing safety features that are not possible in older mechanical tourniquets. These systems can monitor the cuff inflation time as well as regulate the cuff pressure to a known pressure throughout the surgical procedure. Some microprocessor controlled tourniquets are capable of calculating the proper pressure to ensure complete blood occlusion in about 30 seconds. This assists the operating room staff in deciding what the tourniquet pressure should be set at on a per-patient basis.
Contoured and wide cuffs
Studies have shown that tourniquet cuff pressure can be substantially reduced by using wide, contoured cuffs. A wider and contoured cuff has more contact with the limb's surface area and disperses the cuff's force. This concept is emerging from the surgical field into the emergency field with wider emergency tourniquets.
Integrated tourniquet cuff testing
The Association of Operative Registered Nurses (AORN) recommends that the tourniquet cuff, tubing, connectors, gauges, and pressure source should be kept clean and in working order. Some modern tourniquet systems are capable of testing these items in 30 seconds.