
Synonyms scarlatina, scarletina ICD-10 A38 OMIM 012541 | Specialty Infectious disease ICD-9-CM 034.1 DiseasesDB 29032 | |
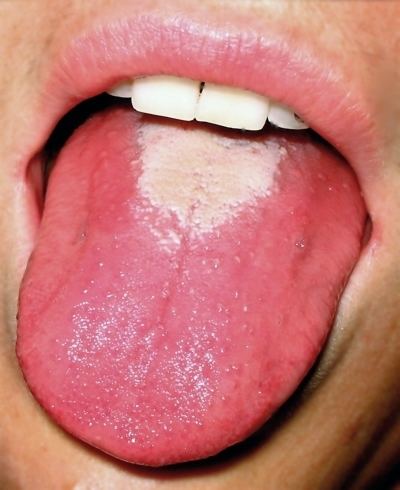 | ||
Scarlet fever can occur as a result of a group A Streptococcus (group A strep) infection. The signs and symptoms include a sore throat, fever, headaches, swollen lymph nodes, and a characteristic rash. The rash is red and feels like sandpaper and the tongue may be red and bumpy. It most commonly affects children between five and fifteen years of age.
Contents
- Signs and symptoms
- Rash
- Other features
- Course
- Pathophysiology
- Microbiology
- Diagnosis
- Differential diagnosis
- Vaccines
- Treatment
- Antibiotic resistance
- Complications
- Epidemiology
- History
- Dick test and vaccine
- References
Scarlet fever affects a small number of people who have either strep throat or streptococcal skin infections. The bacteria are usually spread by people coughing or sneezing. It can also be spread when a person touches an object that has the bacteria on it and then touches their mouth or nose. The characteristic rash is due to the erythrogenic toxin, a substance produced by some types of the bacterium. The diagnosis is typically confirmed by culturing the throat.
There is no vaccine. Prevention is by frequent handwashing, not sharing personal items, and staying away from other people when sick. The disease is treatable with antibiotics which prevents most complications. Outcomes with scarlet fever are typically good. Long-term complications as a result of scarlet fever include: kidney disease, rheumatic heart disease, and arthritis. It was a leading cause of death in children in the early 20th century.
Signs and symptoms
Scarlet fever is characterized by:
Rash
The rash is the most striking sign of scarlet fever. It usually appears first on the neck and face (often leaving a clear, unaffected area around the mouth). It looks like a bad sunburn with tiny bumps, and it may itch. It then spreads to the chest and back and finally to the rest of the body. In the body creases, especially around the underarms and elbows, the rash forms the classic red streaks known as Pastia's lines. On very dark skin, the streaks may appear darker than the rest of the skin. Areas of rash usually turn white (or paler brown, with dark complexioned skin) when pressed on. By the sixth day of the infection, the rash usually fades, but the affected skin may begin to peel.
Other features
Usually, other symptoms help to confirm a diagnosis of scarlet fever, including a reddened and sore throat, a fever at or above 38 °C (100.4 °F), and swollen glands in the neck. Scarlet fever can also occur with a low fever. The tonsils and back of the throat may have a whitish coating, or appear red, swollen, and dotted with whitish or yellowish specks of pus. Early in the infection, the tongue may have a whitish or yellowish coating. Also, an infected person may have chills, body aches, nausea, vomiting, and loss of appetite.
In rare cases, scarlet fever may develop from a streptococcal skin infection like impetigo. In these cases, the person may not develop soreness of the throat.
Course
When scarlet fever occurs because of a throat infection, the fever typically subsides within 3 to 5 days, and the sore throat passes soon afterward. The scarlet-fever rash usually fades on the sixth day after sore-throat symptoms started, and begins to peel (as described above). The infection itself is usually cured with a 10-day course of antibiotics, but it may take a few weeks for tonsils and swollen glands to return to normal.
Pathophysiology
Scarlet fever is usually spread by the aerosol route (inhalation), but may also be spread by skin contact or by fomites. Although it is not normally considered a food-borne illness, an outbreak of scarlet fever due to infected chicken meat has been reported in China.
Asymptomatic carriage may occur in 15–20% of school-age children.
The incubation period is 1–4 days.
Microbiology
The disease is caused by secretion of pyrogenic exotoxins by the infecting Streptococcus bacteria. Streptococcal pyrogenic exotoxin A (speA) is probably the best studied of these toxins. It is carried by the bacteriophage T12 which integrates into the streptococcal genome from where the toxin is transcribed. The phage itself integrates into a serine tRNA gene on the chromosome.
The T12 virus itself has not been placed into a taxon by the International Committee on Taxonomy of Viruses. It has a double-stranded DNA genome and on morphological grounds appears to be a member of the Siphoviridae.
The speA gene was cloned and sequenced in 1986. It is 753 base pairs in length and encodes a 29.244 kiloDalton (kDa) protein. The protein contains a putative 30- amino-acid signal peptide; removal of the signal sequence gives a predicted molecular weight of 25.787 kDa for the secreted protein. Both a promoter and a ribosome binding site (Shine-Dalgarno sequence) are present upstream of the gene. A transcriptional terminator is located 69 bases downstream from the translational termination codon. The carboxy terminal portion of the protein exhibits extensive homology with the carboxy terminus of Staphylococcus aureus enterotoxins B and C1.
Streptococcal phages other than T12 may also carry the speA gene.
Diagnosis
Scarlet fever can be diagnosed by clinical signs and symptoms. Complete blood count findings characteristic of scarlet fever show a marked increase in white blood cell count with neutrophilia and conserved or increased eosinophils, high erythrocyte sedimentation rate and C-reactive protein (both indications of inflammation), and elevation of antistreptolysin O titer. Blood culture is rarely positive, but the streptococci can usually be demonstrated in throat culture.
Differential diagnosis
Cases need to be differentiated from Far East scarlet-like fever, an infectious disease first reported in the 1950s from Russia. Because of its similar clinical presentation to scarlet fever, it was initially thought to be caused by a Streptococcus. It is now known to be caused by a Gram negative bacillus—Yersinia pseudotuberculosis.
Kawasaki's disease is another important differential, especially in its incomplete form. Scarlet fever appears similar to Kawasaki's disease in some aspects, but lacks the eye signs or the swollen, red fingers and toes. However, the signs of Kawasaki's disease may manifest over a few days, rather than at initial presentation. Complications of missed Kawasaki's disease are significant but rare, and include a 1–2% death rate and coronary artery aneurysms.
Vaccines
No vaccines protect against S. pyogenes infection. A vaccine developed by George and Gladys Dick in 1924 was discontinued due to poor efficacy and the introduction of antibiotics. Difficulties in vaccine development include the considerable strain variety of S. pyogenes present in the environment and the amount of time and number of people needed for appropriate trials for safety and efficacy of any potential vaccine.
There used to be a diphtheria scarlet fever vaccine. It was, however, found not to be effective. This product was discontinued by the end of World War II.
Treatment
The treatment and course of scarlet fever is the same as that of strep throat.
Antibiotic resistance
A drug-resistant strain of scarlet fever, resistant to macrolide antibiotics such as erythromycin, but retaining drug-sensitivity to beta-lactam antibiotics such as penicillin, emerged in Hong Kong in 2011, accounting for at least two deaths in that city—the first such in over a decade. About 60% of circulating strains of the group A Streptococcus that cause scarlet fever in Hong Kong are resistant to macrolide antibiotics, says Professor Kwok-yung Yuen, head of Hong Kong University's microbiology department. Previously, observed resistance rates had been 10–30%; the increase is likely the result of overuse of macrolide antibiotics in recent years.
Complications
The complications of scarlet fever include septic complications due to spread of streptococci in blood, and immune-mediated complications due to an aberrant immune response. Septic complications—today rare—include ear and sinus infection, streptococcal pneumonia, empyema thoracis, meningitis, and full-blown sepsis, upon which the condition may be called malignant scarlet fever.
Immune complications include acute glomerulonephritis, rheumatic fever, and erythema nodosum. The secondary scarlatinous disease, or secondary malignant syndrome of scarlet fever, includes renewed fever, renewed angina, septic ear, nose, and throat complications, and kidney infection or rheumatic fever, and is seen around the 18th day of untreated scarlet fever.
An association between scarlet fever and hepatitis has been recognized for several decades. The causal mechanism is unknown.
Epidemiology
This disease is most common in children ages 5–15; males and females are equally affected. By the age of 10 years, 80% of children have acquired protective antibodies against streptococcal pyrogenic exotoxins, preventing development of scarlet fever.
History
It is unclear when a description of this disease was first recorded. Hippocrates, writing around 400 BC, described the condition of a patient with a sore throat and skin ulcers, but it is not entirely clear from his description whether the patient had scarlet fever. In the 10th and 11th centuries, the physicians Rhazes, Ali Abbas, and Avicenna described an illness that was measles-like, but with a more vivid colour and more dangerous. Again, it is not certain that these descriptions refer to scarlet fever.
The first description of the disease in the medical literature appeared in the 1553 book De Tumoribus praeter Naturam by the Sicilian anatomist and physician Giovanni Filippo Ingrassia, where he referred to it as rossalia or rosania. It was redescribed by Johann Weyer during an epidemic in lower Germany between 1564 and 1565; he referred to it as scalatina anginosa. The first unequivocal description of scarlet fever appeared in a book by Joannes Coyttarus of Poitiers, De febre purpura epidemiale et contagiosa libri duo, which was published in 1578 in Paris. Daniel Sennert of Wittenberg described the classical 'scarlatinal desquamation' in 1572 and was also the first to describe the early arthritis, scarlatinal dropsy, and ascites associated with the disease.
In 1827, Bright was the first to recognize the involvement of the renal system in scarlet fever.
The association between streptococci and disease was first described in 1874 by Billroth, discussing patients with wound infections. Billroth also coined the genus name Streptococcus. The organism was first cultured in 1883 by the German surgeon Friedrich Fehleisen. He cultured it from perierysipelas lesions. Rosenbach gave the organism its current name (Streptococcus pyogenes) in 1884.
Also in 1884, the German physician Friedrich Loeffler was the first to show the presence of streptococci in the throats of patients with scarlet fever. Because not all patients with pharyngeal streptococci developed scarlet fever, these findings remained controversial for some time. The association between streptococci and scarlet fever was confirmed by Alphonse Dochez and George and Gladys Dick in the early 1900s.
Nil Filatow (in 1895) and Clement Dukes (in 1894) described an exantematous disease which they thought was a form of rubella, but in 1900, Dukes described it as a separate illness which came to be known as Dukes' disease, Filatov’s disease, or fourth disease. However, in 1979, Keith Powell identified it as in fact the same illness as the form of scarlet fever that is caused by staphylococcal exotoxin and is known as staphylococcal scalded skin syndrome.
Scarlet fever serum from horses was used in the treatment of children beginning in 1900 and reduced mortality rates significantly.
In 1906, the Austrian pediatrician Clemens von Pirquet postulated that disease-causing immune complexes were responsible for the nephritis that followed scarlet fever.
Bacteriophages were discovered in 1915 by Frederick Twort. His work was overlooked and bacteriophages were later rediscovered by Felix d'Herelle in 1917. The specific association of scarlet fever with the group A streptococci had to await the development of Lancefield's streptococcal grouping scheme in the 1920s. George and Gladys Dick showed that cell-free filtrates could induce the erythematous reaction characteristic of scarlet fever, proving that this reaction was due to a toxin. Karelitz and Stempien discovered that extracts from human serum globulin and placental globulin can be used as lightening agents for scarlet fever and this was used later as the basis for the Dick test. The association of scarlet fever and bacteriophages was described in 1926 by Cantucuzene and Boncieu.
The discovery of penicillin and its subsequent widespread use has significantly reduced the mortality of this once feared disease.
The first toxin that causes this disease was cloned and sequenced in 1986 by Weeks and Ferretti.
Dick test and vaccine
The Dick test was invented in 1924 and was used to identify those susceptible to scarlet fever. A broth culture filtrate from an erythrogenic toxin-producing group A streptococcus was injected intracutaneously into susceptible persons. In those susceptible, erythematous and oedematous skin reactions developed by 24 hours after injection. A second injection of antitoxin into the site neutralized the reactions. Nonreactors were considered to have sufficient antibodies to the toxin, and thus were not susceptible to scarlet fever.
Gladys Henry Dick and George Frederick Dick developed a vaccine in 1924 that was later eclipsed by penicillin in the 1940s. Broth filtrates were used as the basis for the patent the Dicks took out on their vaccine in 1924 in the United Kingdom and in 1925 in the United States.