
 | ||
The "prism cover test" (PCT), is an objective measurement and the gold standard in measuring strabismus, i.e. ocular misalignment, or a deviation of the eye. It is used by ophthalmologists and orthoptists in order to measure the vertical and horizontal deviation and includes both manifest and latent components. Manifest is defined by the eye deviating constantly or intermittently, where-as latent is where the deviation is normally controlled but becomes present when the eyes are dissociated. A PCT reveals the total deviation and cannot distinguish between latent and manifest strabismus as you are using an alternate cover test.
Contents
- Indicated in
- Not indicated in
- Advantages
- Disadvantages
- Method
- Recording
- Examples of recording
- Interpretation
- Considerations
- References
A number of different instruments are required when performing a PCT.
These include:
In order to perform a PCT, you must first perform a cover test as this gives an estimation of the size of the strabismus, thus an approximate starting point on the prism bar. You can also get an indication of presence and type of strabismus by observing the patients’ eye and observing corneal reflections, also known as Hirschbergs. It also shows whether the patient has a manifest or latent deviation. If a manifest deviation is present, it reveals which eye has the deviation or if it is alternating between both eyes.
Indicated in
Not indicated in
Advantages
Disadvantages
Method
The prism cover test must be conducted at near (33 cm), at distance (6m) and if necessary at greater than 6 metres. Before commencing the test, ensure the patient is sitting upright with their chin and head straight. Patients with a head tilt (abnormal head posture) are ‘not formally controlled by using a bite bar or chin rest’ and are always tested with their head tilt and then without their head tilt
The results leading on from the cover test will give you an indication of the type of deviation and which way you should hold your prism for the next stage of the test. Either BASE IN for an exodeviation (eye turned out), BASE OUT for an esodeviation (eye turned in), BASE UP for a hypodeviation (eye turned down) or BASE DOWN for a hyperdeviation (eye turned up).
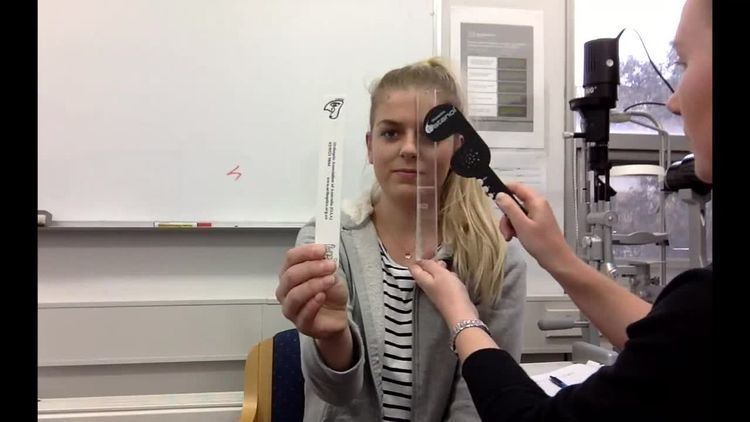
Steps: 1. The patient should be measured in primary position first and then in any other positions of gaze of concern. For near fixation, the patient should hold an accommodative target (fixation stick) at 33 cm, ensuring it is in line with their visual axis. By having the patient read out loud the letters at the top of the fixation stick, it is easy to ensure they are maintaining their accommodation.
2. The examiner then holds the prism bar over the patients deviating eye, starting at a small strength prism, however, if the deviation on the cover test appeared to be large, a larger strength prism may be used to achieve results quicker.
3. With the prism present, an alternate cover test is performed. It is important that an alternate cover test is performed correctly in order to ensure maximum dissociation as we are determining the total deviation size which includes both latent and manifest.
Note: It is important to ensure the patient maintains good fixation, by continuing to look at the near fixation stick.
4. As the alternate cover test is performed, the examiner watches the patients eye for movement. If movement is seen, the prism bar is moved to increase the power. If the ‘deviation exceeds 50 prism dioptres, such that a single prism bar cannot be used’, prisms can either be stacked or split
5. Prism strength is increased until the eye under the prism produces no movement, meaning the deviation is neutralised.
6. To confirm neutralisation the next prism of increasing strength should produce a movement in the opposite direction indicating overcorrection.
7. Once the results for the near PCT have been recorded, the procedure should be repeated at 6m with the Snellen chart and if needed at greater than 6m by patient fixating out the window.
8. Continue the test until neutralisation has been established.
Recording
The PCT recordings assist in classification and diagnosis of specific strabismic conditions by comparing the size of the deviation from near to distance and also in other various positions of gaze.
When recording the results obtained on a PCT it must be noted:
Examples of recording
PCT cc (D) 12 p.d BI 6 p.d BU (FL) (N) 18 p.d BI 6 p.d BU (FL)or
PCT cc (D) 12 p.d BI R/L 6 p.d (FR&L) (N) 18 p.d BI R/L 6 p.d (FR&L)Interpretation
In the first example, it has been noted that when conducting the PCT, this patient wore correction, was fixing left and has a twelve prism dioptre exotropia in the distance. At near they have a larger exotropic deviation measuring 18 prism dioptres. They also have a right hypertropia of six prism dioptres. This means that when the PCT was performed, the deviating eye was neutralised and no movement was seen at these points on the prism bar.