
Specialty Gynecology ICD-9-CM 256.4 MedlinePlus 000369 | ICD-10 E28.2 OMIM 184700 | |
 | ||
Synonyms hyperandrogenic anovulation (HA), Stein–Leventhal syndrome | ||
Polycystic ovary syndrome (PCOS) is a set of symptoms due to elevated androgens (male hormones) in women. Signs and symptoms of PCOS include irregular or no menstrual periods, heavy periods, excess body and facial hair, acne, pelvic pain, difficulty getting pregnant, and patches of thick, darker, velvety skin. Associated conditions include type 2 diabetes, obesity, obstructive sleep apnea, heart disease, mood disorders, and endometrial cancer.
Contents
- Signs and symptoms
- Cause
- Diagnosis
- Definition
- NIH
- Rotterdam
- Standard diagnostic assessments
- Associated conditions
- Differential diagnosis
- Pathogenesis
- Management
- Diet
- Medications
- Infertility
- Hirsutism and acne
- Menstrual irregularity
- Alternative medicine
- Prognosis
- Epidemiology
- History
- Names
- References
PCOS is due to a combination of genetic and environmental factors. Risk factors include obesity, not enough physical exercise, and a family history of someone with the condition. Diagnosis is based on two of the following three findings: no ovulation, high androgen levels, and ovarian cysts. Cysts may be detectable by ultrasound. Other conditions that produce similar symptoms include adrenal hyperplasia, hypothyroidism, and hyperprolactinemia.
PCOS has no cure. Treatment may involve lifestyle changes such as weight loss and exercise. Birth control pills may help with improving the regularity of periods, excess hair growth, and acne. Metformin and anti-androgens may also help. Other typical acne treatments and hair removal techniques may be used. Efforts to improve fertility include weight loss, clomiphene, or metformin. In vitro fertilization is used by some in whom other measures are not effective.
PCOS is the most common endocrine disorder among women between the ages of 18 and 44. It affects approximately 2% to 20% of this age group depending on how it is defined. It is one of the leading causes of poor fertility. The earliest known description of what is now recognized as PCOS dates from 1721 in Italy.
Signs and symptoms
Common signs and symptoms of PCOS include the following:
Asians affected by PCOS are less likely to develop hirsutism than those of other ethnic backgrounds.
Cause
PCOS is a heterogeneous disorder of uncertain cause. There is some evidence that it is a genetic disease. Such evidence includes the familial clustering of cases, greater concordance in monozygotic compared with dizygotic twins and heritability of endocrine and metabolic features of PCOS.
The genetic component appears to be inherited in an autosomal dominant fashion with high genetic penetrance but variable expressivity in females; this means that each child has a 50% chance of inheriting the predisposing genetic variant(s) from a parent, and, if a daughter receives the variant(s), the daughter will have the disease to some extent. The genetic variant(s) can be inherited from either the father or the mother, and can be passed along to both sons (who may be asymptomatic carriers or may have symptoms such as early baldness and/or excessive hair) and daughters, who will show signs of PCOS. The phenotype appears to manifest itself at least partially via heightened androgen levels secreted by ovarian follicle theca cells from women with the allele. The exact gene affected has not yet been identified. In rare instances, single-gene mutations can give rise to the phenotype of the syndrome. Current understanding of the pathogenesis of the syndrome suggests, however, that it is a complex multigenic disorder.
The severity of PCOS symptoms appears to be largely determined by factors such as obesity.
PCOS has some aspects of a metabolic disorder, since its symptoms are partly reversible. Even though considered as a gynecological problem, PCOS consists of 28 clinical symptoms.
Even though the name suggests that the ovaries are central to disease pathology, cysts are a symptom instead of the cause of the disease. Some symptoms of PCOS will persist even if both ovaries are removed; the disease can appear even if cysts are absent. Since its first description by Stein and Leventhal in 1935, the criteria of diagnosis, symptoms, and causative factors are subject to debate. Gynecologists often see it as a gynecological problem, with the ovaries being the primary organ affected. However, recent insights show a multisystem disorder, with the primary problem lying in hormonal regulation in the hypothalamus, with the involvement of many organs. The name PCOD is used when there is ultrasonographic evidence. The term PCOS is used since there is a wide spectrum of symptoms possible, and cysts in the ovaries are seen only in 15% of people.
PCOS may be related to or worsened by exposures during the prenatal period, epigenetic factors, environmental impacts (especially industrial endocrine disruptors such as bisphenol A and certain drugs) and the increasing rates of obesity.
Diagnosis
Not everyone with PCOS has polycystic ovaries (PCO), nor does everyone with ovarian cysts have PCOS; although a pelvic ultrasound is a major diagnostic tool, it is not the only one. The diagnosis is straightforward using the Rotterdam criteria, even when the syndrome is associated with a wide range of symptoms.
Definition
Two definitions are commonly used:
NIH
In 1990 a consensus workshop sponsored by the NIH/NICHD suggested that a person has PCOS if they have all of the following:- oligoovulation
- signs of androgen excess (clinical or biochemical)
- exclusion of other disorders that can result in menstrual irregularity and hyperandrogenism
Rotterdam
In 2003 a consensus workshop sponsored by ESHRE/ASRM in Rotterdam indicated PCOS to be present if any 2 out of 3 criteria are met, in the absence of other entities that might cause these findings- oligoovulation and/or anovulation
- excess androgen activity
- polycystic ovaries (by gynecologic ultrasound)
The Rotterdam definition is wider, including many more women, the most notable ones being women without androgen excess. Critics say that findings obtained from the study of women with androgen excess cannot necessarily be extrapolated to women without androgen excess.
- excess androgen activity
- oligoovulation/anovulation and/or polycystic ovaries
- exclusion of other entities that would cause excess androgen activity
Standard diagnostic assessments
Some other blood tests are suggestive but not diagnostic. The ratio of LH (Luteinizing hormone) to FSH (Follicle-stimulating hormone), when measured in international units, is elevated in women with PCOS. Common cut-offs to designate abnormally high LH/FSH ratios are 2:1 or 3:1 as tested on Day 3 of the menstrual cycle. The pattern is not very sensitive; a ratio of 2:1 or higher was present in less than 50% of women with PCOS in one study. There are often low levels of sex hormone-binding globulin, in particular among obese or overweight women.
Anti-Müllerian hormone (AMH) is increased in PCOS, and may become part of its diagnostic criteria.
Associated conditions
Differential diagnosis
Other causes of irregular or absent menstruation and hirsutism, such as hypothyroidism, congenital adrenal hyperplasia (21-hydroxylase deficiency), Cushing's syndrome, hyperprolactinemia, androgen secreting neoplasms, and other pituitary or adrenal disorders, should be investigated.
Pathogenesis
Polycystic ovaries develop when the ovaries are stimulated to produce excessive amounts of androgenic hormones, in particular testosterone, by either one or a combination of the following (almost certainly combined with genetic susceptibility):
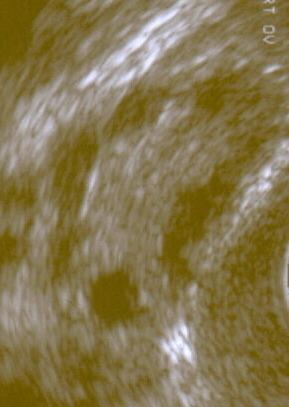
The syndrome acquired its most widely used name due to the common sign on ultrasound examination of multiple (poly) ovarian cysts. These "cysts" are actually immature follicles not cysts. The follicles have developed from primordial follicles, but the development has stopped ("arrested") at an early antral stage due to the disturbed ovarian function. The follicles may be oriented along the ovarian periphery, appearing as a 'string of pearls' on ultrasound examination.
Women with PCOS experience an increased frequency of hypothalamic GnRH pulses, which in turn results in an increase in the LH/FSH ratio.
A majority of women with PCOS have insulin resistance and/or are obese. Their elevated insulin levels contribute to or cause the abnormalities seen in the hypothalamic-pituitary-ovarian axis that lead to PCOS. Hyperinsulinemia increases GnRH pulse frequency, LH over FSH dominance, increased ovarian androgen production, decreased follicular maturation, and decreased SHBG binding. Furthermore, excessive insulin, acting through its cognate receptor in the presence of component cAMP signalling, upregulates 17α-hydroxylase activity via PI3K, 17α-hydroxylase activity being responsible for synthesising androgen precursors. The combined effects of hyperinsulinemia contribute to an increased risk of PCOS. Insulin resistance is a common finding among women with a normal weight as well as overweight women.
Adipose tissue possesses aromatase, an enzyme that converts androstenedione to estrone and testosterone to estradiol. The excess of adipose tissue in obese women creates the paradox of having both excess androgens (which are responsible for hirsutism and virilization) and estrogens (which inhibits FSH via negative feedback).
PCOS may be associated with chronic inflammation, with several investigators correlating inflammatory mediators with anovulation and other PCOS symptoms. Similarly, there seems to be a relation between PCOS and increased level of oxidative stress.
It has previously been suggested that the excessive androgen production in PCOS could be caused by a decreased serum level of IGFBP-1, in turn increasing the level of free IGF-I, which stimulates ovarian androgen production, but recent data concludes this mechanism to be unlikely.
PCOS has also been associated with a specific FMR1 sub-genotype. The research suggests that women with heterozygous-normal/low FMR1 have polycystic-like symptoms of excessive follicle-activity and hyperactive ovarian function.
Transgender men may experience a higher than expected rate of PCOS due to increased testosterone, if they choose to take hormone therapy as part of their gender presentation.
Management
The primary treatments for PCOS include: lifestyle changes, medications and surgery.
Goals of treatment may be considered under four categories:
In each of these areas, there is considerable debate as to the optimal treatment. One of the major reasons for this is the lack of large-scale clinical trials comparing different treatments. Smaller trials tend to be less reliable and hence may produce conflicting results.
General interventions that help to reduce weight or insulin resistance can be beneficial for all these aims, because they address what is believed to be the underlying cause.
As PCOS appears to cause significant emotional distress, appropriate support may be useful.
Diet
Where PCOS is associated with overweight or obesity, successful weight loss is the most effective method of restoring normal ovulation/menstruation, but many women find it very difficult to achieve and sustain significant weight loss. A scientific review in 2013 found similar decreases in weight and body composition and improvements in pregnancy rate, menstrual regularity, ovulation, hyperandrogenism, insulin resistance, lipids, and quality of life to occur with weight loss independent of diet composition. Still, a low GI diet, in which a significant part of total carbohydrates are obtained from fruit, vegetables, and whole-grain sources, has resulted in greater menstrual regularity than a macronutrient-matched healthy diet.
Vitamin D deficiency may play some role in the development of the metabolic syndrome, so treatment of any such deficiency is indicated. However, a systematic review of 2015 found no evidence that vitamin D supplementation reduced or mitigated metabolic and hormonal dysregulations in PCOS. As of 2012, interventions using dietary supplements to correct metabolic deficiencies in people with PCOS had been tested in small, uncontrolled and nonrandomized clinical trials; the resulting data is insufficient to recommend their use.
Medications
Medications for PCOS include oral contraceptives and metformin. The oral contraceptives increase sex hormone binding globulin production, which increases binding of free testosterone. This reduces the symptoms of hirsutism caused by high testosterone and regulates return to normal menstrual periods. Metformin is a drug commonly used in type 2 diabetes to reduce insulin resistance, and is used off label (in the UK, US, AU and EU) to treat insulin resistance seen in PCOS. In many cases, metformin also supports ovarian function and return to normal ovulation. Spironolactone can be used for its antiandrogenic effects, and the topical cream eflornithine can be used to reduce facial hair. A newer insulin resistance drug class, the thiazolidinediones (glitazones), have shown equivalent efficacy to metformin, but metformin has a more favorable side effect profile. The United Kingdom's National Institute for Health and Clinical Excellence recommended in 2004 that women with PCOS and a body mass index above 25 be given metformin when other therapy has failed to produce results. Metformin may not be effective in every type of PCOS, and therefore there is some disagreement about whether it should be used as a general first line therapy. The use of statins in the management of underlying metabolic syndrome remains unclear.
It can be difficult to become pregnant with PCOS because it causes irregular ovulation. Medications to induce fertility when trying to conceive include the ovulation inducer clomiphene or pulsatile leuprolide. Metformin improves the efficacy of fertility treatment when used in combination with clomiphene. Metformin is thought to be safe to use during pregnancy (pregnancy category B in the US). A review in 2014 concluded that the use of metformin does not increase the risk of major birth defects in women treated with metformin during the first trimester.
Infertility
Not all women with PCOS have difficulty becoming pregnant. For those that do, anovulation or infrequent ovulation is a common cause. Other factors include changed levels of gonadotropins, hyperandrogenemia and hyperinsulinemia. Like women without PCOS, women with PCOS that are ovulating may be infertile due to other causes, such as tubal blockages due to a history of sexually transmitted diseases.
For overweight, anovulatory women with PCOS, weight loss and diet adjustments, especially to reduce the intake of simple carbohydrates, are associated with resumption of natural ovulation.
For those women that after weight loss still are anovulatory or for anovulatory lean women, then the ovulation-inducing medications clomiphene citrate and FSH are the principal treatments used to promote ovulation. Previously, the anti-diabetes medication metformin was recommended treatment for anovulation, but it appears less effective than clomiphene.
For women not responsive to clomiphene and diet and lifestyle modification, there are options available including assisted reproductive technology procedures such as controlled ovarian hyperstimulation with follicle-stimulating hormone (FSH) injections followed by in vitro fertilisation (IVF).
Though surgery is not commonly performed, the polycystic ovaries can be treated with a laparoscopic procedure called "ovarian drilling" (puncture of 4–10 small follicles with electrocautery, laser, or biopsy needles), which often results in either resumption of spontaneous ovulations or ovulations after adjuvant treatment with clomiphene or FSH. (Ovarian wedge resection is no longer used as much due to complications such as adhesions and the presence of frequently effective medications.) There are, however, concerns about the long-term effects of ovarian drilling on ovarian function.
Hirsutism and acne
When appropriate (e.g., in women of child-bearing age who require contraception), a standard contraceptive pill is frequently effective in reducing hirsutism. Progestogens such as norgestrel and levonorgestrel should be avoided due to their androgenic effects.
Other drugs with anti-androgen effects include flutamide, and spironolactone, which can give some improvement in hirsutism. Metformin can reduce hirsutism, perhaps by reducing insulin resistance, and is often used if there are other features such as insulin resistance, diabetes, or obesity that should also benefit from metformin. Eflornithine (Vaniqa) is a drug that is applied to the skin in cream form, and acts directly on the hair follicles to inhibit hair growth. It is usually applied to the face. 5-alpha reductase inhibitors (such as finasteride and dutasteride) may also be used; they work by blocking the conversion of testosterone to dihydrotestosterone (the latter of which responsible for most hair growth alterations and androgenic acne).
Although these agents have shown significant efficacy in clinical trials (for oral contraceptives, in 60–100% of individuals), the reduction in hair growth may not be enough to eliminate the social embarrassment of hirsutism, or the inconvenience of plucking or shaving. Individuals vary in their response to different therapies. It is usually worth trying other drug treatments if one does not work, but drug treatments do not work well for all individuals.
Menstrual irregularity
If fertility is not the primary aim, then menstruation can usually be regulated with a contraceptive pill. The purpose of regulating menstruation, in essence, is for the woman's convenience, and perhaps her sense of well-being; there is no medical requirement for regular periods, as long as they occur sufficiently often.
If a regular menstrual cycle is not desired, then therapy for an irregular cycle is not necessarily required. Most experts say that, if a menstrual bleed occurs at least every three months, then the endometrium (womb lining) is being shed sufficiently often to prevent an increased risk of endometrial abnormalities or cancer. If menstruation occurs less often or not at all, some form of progestogen replacement is recommended. An alternative is oral progestogen taken at intervals (e.g., every three months) to induce a predictable menstrual bleeding.
Alternative medicine
A 2011 review found not enough evidence to conclude any beneficial effect from D-chiro-inositol. A 2012 review, found myo-inositol supplementation, however, appears to be effective in improving several of the hormonal disturbances of PCOS. There is not evidence to support the use of acupuncture for treatment of ovulation disorders in women with PCOS.
Prognosis
A diagnosis of PCOS suggests an increased risk of the following:
Early diagnosis and treatment may reduce the risk of some of these, such as type 2 diabetes and heart disease.
The risk of ovarian cancer and breast cancer is not significantly increased overall.
Epidemiology
The prevalence of PCOS depends on the choice of diagnostic criteria. The World Health Organization estimates that it affects 116 million women worldwide as of 2010 (3.4% of women). One community-based prevalence study using the Rotterdam criteria found that about 18% of women had PCOS, and that 70% of them were previously undiagnosed.
Ultrasonographic findings of polycystic ovaries are found in 8-25% of normal women. 14% women on oral contraceptives are found to have polycystic ovaries. Ovarian cysts are also a common side effect of intrauterine devices (IUDs).
History
The condition was first described in 1935 by American gynecologists Irving F. Stein, Sr. and Michael L. Leventhal, from whom its original name of Stein–Leventhal syndrome is taken.
The earliest published description of a person with what is now recognized as PCOS was in 1721 in Italy. Cyst-related changes to the ovaries were described in 1844.
Names
Other names for this syndrome include polycystic ovary disease, functional ovarian hyperandrogenism, ovarian hyperthecosis, sclerocystic ovary syndrome, and Stein–Leventhal syndrome. The eponymous last option is the original name; it is now used, if at all, only for the subset of women with all the symptoms of amenorrhea with infertility, hirsutism, and enlarged polycystic ovaries.
Most common names for this disease derive from a typical finding on medical images, called a polycystic ovary. A polycystic ovary has an abnormally large number of developing eggs visible near its surface, looking like many small cysts or a string of pearls.