
ICD-9-CM 52.8 MedlinePlus 003007 | MeSH D016035 | |
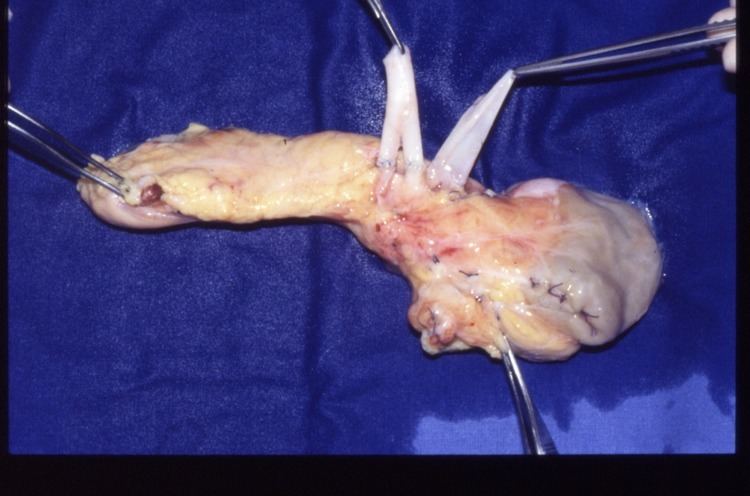 | ||
Kidney pancreas transplants
A pancreas transplant is an organ transplant that involves implanting a healthy pancreas (one that can produce insulin) into a person who usually has diabetes. Because the pancreas is a vital organ, performing functions necessary in the digestion process, the recipient's native pancreas is left in place, and the donated pancreas is attached in a different location. In the event of rejection of the new pancreas, which would quickly cause life-threatening diabetes, there would be a significant chance the recipient would not survive very well for long without the native pancreas, however dysfunctional, still in place. The healthy pancreas comes from a donor who has just died or it may be a partial pancreas from a living donor. At present, pancreas transplants are usually performed in persons with insulin-dependent diabetes, who can develop severe complications. Patients with the most common- and deadliest- form of pancreatic cancer (pancreatic adenomas- which are usually always malignant, with a poor prognosis and high risk for metastasis- as opposed to more treatable pancreatic neuroendocrine tumors or pancreatic insulinomas) are usually not eligible for valuable pancreatic transplantations, since the condition usually has a very high mortality rate and the disease, which is usually highly malignant and detected too late to treat, could and probably would soon return.
Contents
Medical uses
In most cases, pancreas transplantation is performed on individuals with type 1 diabetes with end-stage renal disease, brittle diabetes and hypoglycaemia unawareness. The majority of pancreas transplantation (>90%) are simultaneous pancreas-kidney transplantation. It may also be performed as part of a kidney-pancreas transplantation.
Complications
Complications immediately after surgery include thrombosis, pancreatitis, infection, bleeding and rejection. Rejection may occur immediately or at any time during the patient's life. This is because the transplanted pancreas comes from another organism, thus the recipient's immune system will consider it as an aggression and try to combat it. Organ rejection is a serious condition and ought to be treated immediately. In order to prevent it, patients must take a regimen of immunosuppressive drugs. Drugs are taken in combination consisting normally of ciclosporin, azathioprine and corticosteroids. But as episodes of rejection may reoccur throughout a patient's life, the exact choices and dosages of immunosuppressants may have to be modified over time. Sometimes tacrolimus is given instead of ciclosporin and mycophenolate mofetil instead of azathioprine.
Types
There are four main types of pancreas transplantation:
Preservation until implantation
Standard practice is to replace the donor's blood in the pancreatic tissue with an ice-cold organ storage solution, such as UW (Viaspan) or HTK until the allograft pancreatic tissue is implanted.
Prognosis
The prognosis after pancreas transplantation is very good. Over the recent years, long-term success has improved and risks have decreased. One year after transplantation more than 95% of all patients are still alive and 80-85% of all pancreases are still functional. After transplantation patients need lifelong immunosuppression. Immunosuppression increases the risk for a number of different kinds of infection and cancer.
It is unclear if steroids, which are often used as immunosuppressant, can be replaced with something else.
History
As described by a pioneer in the field, D.E. Sutherland, whole pancreas transplantation began as a part of multi-organ transplants, in the mid-to-late 1960s, at the University of Minnesota:
The first attempt to cure type 1 diabetes by pancreas transplantation was done at the University of Minnesota, in Minneapolis, on December 17, 1966… [This] opened the door to a period, between the mid 70's to mid 80's where only segmental pancreatic grafts were used... In the late 70's-early 80's, three major events… boosted the development of pancreas transplantation… [At] the Spitzingsee meetings, participants had the idea to renew the urinary drainage technique of the exocrine secretion of the pancreatic graft with segmental graft and eventually with whole pancreaticoduodenal transplant. That was clinically achieved during the mid 80's and remained the mainstay technique during the next decade. In parallel, the Swedish group developed the whole pancreas transplantation technique with enteric diversion. It was the onset of the whole pancreas reign. The enthusiasm for the technique was rather moderated in its early phase due to the rapid development of liver transplantation and the need for sharing vascular structures between both organs, liver and pancreas. During the modern era of immunosuppression, the whole pancreas transplantation technique with enteric diversion became the gold standard…
The first pancreas transplantation, performed in a multi-organ transplant with kidney and duodenum, was into a 28-year-old woman; her death three month post-surgery did not obscure the apparent success of the pancreatic replacement. It was performed 1966 by the team of W.D. Kelly, R.C. Lillehei, F.K. Merkel, Y. Idezuki, F.C. Goetz and coworkers at the University Hospitals, University of Minnesota, three years after the first kidney transplantation. The first living-related partial pancreas transplantation was done in 1979.