
ICD-10 D16.9 DiseasesDB 31488 MeSH D010017 | ICD-O 9191/0 eMedicine article/392850 | |
 | ||
An osteoid osteoma is a benign bone tumor that arises from osteoblasts and was originally thought to be a smaller version of an osteoblastoma. Osteoid osteomas tend to be less than 1.5 cm in size. The tumor can be in any bone in the body but are most common in long bones, such as the femur and tibia. They account for 10 to 12 percent of all benign bone tumors. "Osteoid osteomas may occur at any age, and are most common in patients between the ages of 4 and 25 years old. Males are affected approximately three times more commonly than females."
Contents
Presentation
Characterized by being less than 1.5 cm in diameter, osteoid osteomas most frequently occur in young men (Male:Female ratio 3:1) and may occur in any bone of the body, most frequently around the knee but often also seen in the vertebrae, in the long bones and less commonly in the mandible or other craniofacial bones.
Severe pain typically occurs at night, but can also be constant at any time of day. The chief complaint may only be of dull pain which is non radiating and persistent throughout 24 hours but increases significantly at night. Pain tends to be relieved with NSAIDs such as ibuprofen.
Histological Findings
On histological examination osteoid osteoma consists of a small (< 1.52 cm), yellowish to red nidus of osteoid and woven bone with interconnected trabeculae, and a background and rim of highly vascularized, fibrous connective tissue. Varying degrees of sclerotic bone reaction may surround the lesion. Benign osteoblastoma is virtually indistinguishable from osteoid osteoma. The usual appearance included a fibrovascular stroma with numerous osteoblasts, osteoid tissue, well-formed woven bone, and giant cells. The osteoblasts were generally small and regular in shape.
Symptoms
The most common symptoms of an Osteoid Osteoma are:
The most common symptom is pain that can be relieved with over the counter pain medication in the beginning. After the benign tumor develops further the pain can not be alleviated with medication and minor to severe swelling starts to occur. Although, in some cases the pain level remains the same for years, and regular NSAIDs intake keeps the pain at bay. The tumor is often found through x-ray imaging. "Conventional radiographs reveal a well-demarcated lytic lesion (nidus) surrounded by a distinct zone of sclerosis" that allow doctors to identify the tumor.
Diagnosis
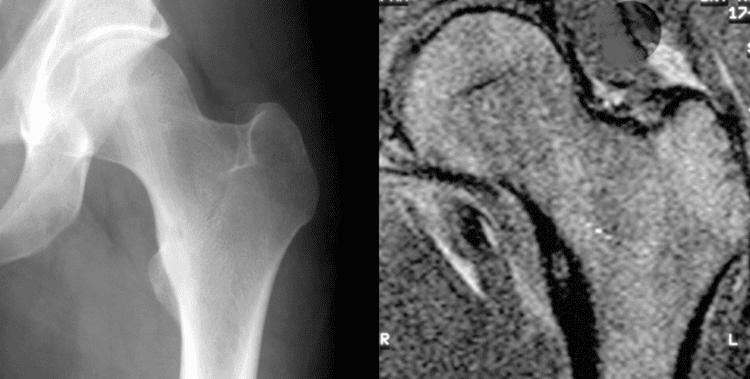
Radiographs in osteoid osteoma typically show a round lucency, containing a dense sclerotic central nidus (the characteristic lesion in this kind of tumor), surrounded by sclerotic bone. The nidus is seldom larger than 1.5 cm.
The lesion can in most cases be detected on CT scan, bone scans and angiograms. Plain radiographs are not always diagnostic. MRI adds little to the CT findings which are useful for localisation. Radionuclide scanning shows intense uptake which is useful for localisation at surgery using a hand held detector, and for confirmation that the entire lesion has been removed.
Treatment
Pain may be relieved by nonsteroidal anti-inflammatory drugs.
Treatment varies based on the health of the patient. If he/she is otherwise healthy and is not significantly bothered by the pain, the tumor is treated symptomatically with anti-inflammatories. If this therapy fails or the location of the tumor could lead to growth disturbances, scoliosis, or osteoarthritis, surgical or percutaneous ablation may be considered. If surgery is preferred, the individual may be referred to a podiatrist or an orthopedic surgeon to perform the procedure. Post-surgery therapy and strengthening may be needed, depending on the tumor location and health of the individual. While shown to be effective, surgical resection has many potential complications, including difficult intraoperative identification of the tumor, local recurrence from incomplete resection, and resection of weight bearing bone that can necessitate prolonged hospital stays and complicate recovery.
Recently, CT guided radiofrequency ablation has emerged as a less invasive alternative to surgical resection. In this technique, which can be performed under conscious sedation, a RF probe is introduced into the tumor nidus through a cannulated needle under CT guidance and heat is applied locally to destroy tumor cells. Since the procedure was first introduced for the treatment of osteoid osteomas in the early 1990s, it has been shown in numerous studies to be less invasive and expensive, to result in less bone destruction and to have equivalent safety and efficacy to surgical techniques, with 66 to 96% of patients reporting freedom from symptoms. While initial success rates with RFA are high, symptom recurrence after RFA treatment has been reported, with some studies demonstrating a recurrence rate similar to that of surgical treatment. As of July 17, 2014, treatment with incisionless surgery utilizing an MRI to guide high-intensity ultrasound waves to destroy a benign bone tumor in the leg has been demonstrated.