
 | ||
Low-density lipoprotein (LDL) is one of the five major groups of lipoprotein. These groups, from least dense (largest particles) to most dense (smallest particles), are chylomicrons, very low-density lipoprotein (VLDL), intermediate-density lipoprotein (IDL), low-density lipoprotein and high-density lipoprotein (HDL).
Contents
- Low density lipoproteins ldl rate my science
- Structure
- Physiology
- Transport into the cell
- Role in the innate immune system
- LDL subtype patterns
- Testing
- Estimation of LDL particles via cholesterol content
- Normal ranges
- Direct measurement of LDL particle concentrations
- Optimal ranges
- Lowering LDL cholesterol
- Pharmaceutical
- Lifestyle
- Antioxidants
- References
Lipoproteins transfer lipids (fats) around the body in the extracellular fluid thereby facilitating fats to be available and taken up by the cells body wide via receptor-mediated endocytosis. Lipoproteins are complex particles composed of multiple proteins, typically 80-100 proteins/particle (organized by a single apolipoprotein B for LDL and the larger particles). A single LDL particle is about 220-275 angstroms in diameter typically transporting 3,000 to 6,000 fat molecules/particle, varying in size according to the number and mix of fat molecules contained within. The lipids carried include all fat molecules with cholesterol, phospholipids, and triglycerides dominant; amounts of each varying considerably. Lipoproteins can be sampled from blood for evaluation of atherosclerosis driving factors.
LDL particles pose a risk for cardiovascular disease when they invade the endothelium and become oxidized, since the oxidized forms are more easily retained by the proteoglycans. A complex set of biochemical reactions regulates the oxidation of LDL particles, chiefly stimulated by presence of necrotic cell debris and free radicals in the endothelium. Increasing concentrations of LDL particles are strongly associated with increasing rates of accumulation of atherosclerosis within the walls of arteries over time, eventually resulting in sudden plaque ruptures, decades later, and triggering clots within the artery opening; these debris & clots narrowing or closing off the opening locally (more commonly microscopic branches distal to plaque rupture locations), i.e. cardiovascular disease, stroke, and other vascular disease complications.
LDL particles (though far different from cholesterol per se) are sometimes referred to as bad cholesterol because they can transport their content of lipid molecules into artery walls, attract macrophages, and thus drive atherosclerosis. In contrast, HDL particles (though far different from cholesterol per se) are often called good cholesterol or healthy cholesterol because they can remove lipid molecules from macrophages in the wall of arteries.
A hereditary form of high LDL is familial hypercholesterolemia (FH). High LDL is termed hyperlipoproteinemia type II (after the dated Fredrickson classification).
Low density lipoproteins ldl rate my science
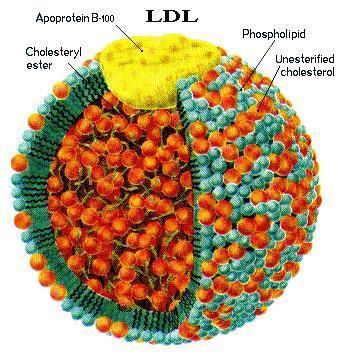
Structure
Each native LDL particle enables emulsification, i.e. surrounding/packaging all fatty acids being carried, enabling these fats to move around the body within the water outside cells. Each particle contains a single apolipoprotein B-100 molecule (Apo B-100, a protein that has 4536 amino acid residues and a mass of 514 kDa), along with 80 to 100 additional ancillary proteins. Each LDL has a highly hydrophobic core consisting of polyunsaturated fatty acid known as linoleate and hundreds to thousands (about 1500 commonly cited as an average) esterified and unesterified cholesterol molecules. This core also carries varying numbers of triglycerides and other fats and is surrounded by a shell of phospholipids and unesterified cholesterol, as well as the single copy of Apo B-100. LDL particles are approximately 22 nm (0.00000087 in.) to 27.5 nm in diameter and have a mass of about 3 million daltons. Since LDL particles contain a variable and changing number of fatty acid molecules, there is a distribution of LDL particle mass and size. Determining the structure of LDL has been a tough task because of its heterogeneous structure. The structure of LDL at human body temperature in native condition, with a resolution of about 16 Angstroms using cryo-electron microscopy, has been recently described.
Physiology
LDL particles are formed as VLDL lipoproteins lose triglyceride through the action of lipoprotein lipase (LPL) and they become smaller and denser (i.e. fewer fat molecules with same protein transport shell), containing a higher proportion of cholesterol esters.
Transport into the cell
When a cell requires additional cholesterol (beyond its current internal HMGCoA production pathway), it synthesizes the necessary LDL receptors as well as PCSK9, a proprotein convertase that marks the LDL receptor for degradation. LDL receptors are inserted into the plasma membrane and diffuse freely until they associate with clathrin-coated pits. When LDL receptors bind LDL particles in the bloodstream, the clathrin-coated pits are endocytosed into the cell.
Vesicles containing LDL receptors bound to LDL are delivered to the endosome. In the presence of low pH, such as that found in the endosome, LDL receptors undergo a conformation change, releasing LDL. LDL is then shipped to the lysosome, where cholesterol esters in the LDL are hydrolysed. LDL receptors are typically returned to the plasma membrane, where they repeat this cycle. If LDL receptors bind to PCSK9, however, transport of LDL receptors is redirected to the lysosome, where they are degraded.
Role in the innate immune system
LDL interfere with the quorum sensing system that upregulates genes required for invasive Staphylococcus aureus infection. The mechanism of antagonism entails binding Apolipoprotein B to a S. aureus autoinducer pheromone, preventing signaling through its receptor. Mice deficient in apolipoprotein B are more susceptible to invasive bacterial infection.
LDL subtype patterns
LDL particles vary in size and density, and studies have shown that a pattern that has more small dense LDL particles, called Pattern B, equates to a higher risk factor for coronary heart disease (CHD) than does a pattern with more of the larger and less-dense LDL particles (Pattern A). This is thought to be because the smaller particles are more easily able to penetrate the endothelium. Pattern I, for intermediate, indicates that most LDL particles are very close in size to the normal gaps in the endothelium (26 nm). According to one study, sizes 19.0–20.5 nm were designated as pattern B and LDL sizes 20.6–22 nm were designated as pattern A.
Some in the medical community have suggested the correspondence between Pattern B and CHD is stronger than the correspondence between the LDL number measured in the standard lipid profile test. Tests to measure these LDL subtype patterns have been more expensive and not widely available, so the common lipid profile test is used more often.
There has also been noted a correspondence between higher triglyceride levels and higher levels of smaller, denser LDL particles and alternately lower triglyceride levels and higher levels of the larger, less dense (a.k.a. "buoyant") LDL.
With continued research, decreasing cost, greater availability and wider acceptance of other lipoprotein subclass analysis assay methods, including NMR spectroscopy, research studies have continued to show a stronger correlation between human clinically obvious cardiovascular events and quantitatively measured particle concentrations.
Testing
Blood tests commonly report LDL-C: the amount of cholesterol which is estimated to be contained with LDL particles, on average, using a formula, the Friedewald equation. In clinical context, mathematically calculated estimates of LDL-C are commonly used as an estimate of how much low density lipoproteins are driving progression of atherosclerosis. The problem with this approach is that LDL-C values are commonly discordant with both direct measurements of LDL-particles and actual rates of atherosclerosis progression.
Direct LDL measurements are also available and better reveal individual issues but are less often promoted or done due to slightly higher costs and being available from only a couple of laboratories in the United States. In 2008, the ADA and ACC recognized direct LDL particle measurement by NMR as superior for assessing individual risk of cardiovascular events.
Estimation of LDL particles via cholesterol content
Chemical measures of lipid concentration have long been the most-used clinical measurement, not because they have the best correlation with individual outcome, but because these lab methods are less expensive and more widely available.
The lipid profile does not measure LDL particles. It only estimates them using the Friedewald equation by subtracting the amount of cholesterol associated with other particles, such as HDL and VLDL, assuming a prolonged fasting state, etc.:
There are limitations to this method, most notably that samples must be obtained after a 12 to 14 h fast and that LDL-C cannot be calculated if plasma triglyceride is >4.52 mmol/L (400 mg/dL). Even at triglyceride levels 2.5 to 4.5 mmol/L, this formula is considered inaccurate. If both total cholesterol and triglyceride levels are elevated then a modified formula, with quantities in mg/dl, may be used
This formula provides an approximation with fair accuracy for most people, assuming the blood was drawn after fasting for about 14 hours or longer, but does not reveal the actual LDL particle concentration because the percentage of fat molecules within the LDL particles which are cholesterol varies, as much as 8:1 variation.
However, the concentration of LDL particles, and to a lesser extent their size, has a stronger and consistent correlation with individual clinical outcome than the amount of cholesterol within LDL particles, even if the LDL-C estimation is approximately correct. There is increasing evidence and recognition of the value of more targeted and accurate measurements of LDL particles. Specifically, LDL particle number (concentration), and to a lesser extent size, have shown slightly stronger correlations with atherosclerotic progression and cardiovascular events than obtained using chemical measures of the amount of cholesterol carried by the LDL particles. It is possible that the LDL cholesterol concentration can be low, yet LDL particle number high and cardiovascular events rates are high. Correspondingly, it is possible that LDL cholesterol concentration can be relatively high, yet LDL particle number low and cardiovascular events are also low. If LDL particle concentration is used to predict cardiovascular events, many other correlates of these clinical outcomes, such as diabetes mellitus, obesity and smoking, lose most of their predictive accuracy.
Normal ranges
In the USA, the American Heart Association, NIH, and NCEP provide a set of guidelines for fasting LDL-Cholesterol levels, estimated or measured, and risk for heart disease. As of about 2005, these guidelines were:
Over time, with more clinical research, these recommended levels keep being reduced because LDL reduction, including to abnormally low levels, was the most effective strategy for reducing cardiovascular death rates in one large double blind, randomized clinical trial of men with hypercholesterolemia; far more effective than coronary angioplasty/stenting or bypass surgery
For instance, for people with known atherosclerosis diseases, the 2004 updated American Heart Association, NIH and NCEP recommendations are for LDL levels to be lowered to less than 70 mg/dL, unspecified how much lower. This low level of less than 70 mg/dL (higher than Tim Russert's value shortly prior to his heart attack) was recommended for primary prevention of 'very-high risk patients' and in secondary prevention as a 'reasonable further reduction'. Lack of evidence for such a recommendation is discussed in an article in the Annals of internal medicine. It should also be noted that statin drugs involved in such clinical trials have numerous physiological effects beyond simply the reduction of LDL levels.
It has been estimated from the results of multiple human pharmacologic LDL lowering trials that LDL should be lowered to below 30 to reduce cardiovascular event rates to near zero. For reference, from longitudinal population studies following progression of atherosclerosis-related behaviors from early childhood into adulthood, it has been discovered that the usual LDL in childhood, before the development of fatty streaks, is about 35 mg/dL. However, all the above values refer to chemical measures of lipid/cholesterol concentration within LDL, not measured low-density lipoprotein concentrations, the accurate approach.
The feasibility of these figures has been questioned by sceptics, claiming that many members of the AHA and NIH are heavily associated with pharmaceutical companies giving them bias towards lowering cholesterol levels and such guidelines giving rise to increased use of cholesterol lowering medicine such as statins.
A study was conducted measuring the effects of guideline changes on LDL cholesterol reporting and control for diabetes visits in the US from 1995 to 2004. It was found that although LDL cholesterol reporting and control for diabetes and coronary heart disease visits improved continuously between 1995 and 2004, neither the 1998 ADA guidelines nor the 2001 ATP III guidelines increased LDL cholesterol control for diabetes relative to coronary heart disease.
Moreover, there are publications regarding the risks of low-LDL cholesterol too.
Direct measurement of LDL particle concentrations
There are several competing methods for measurement of lipoprotein particle concentrations and size. The evidence is that the NMR methodology (developed, automated & greatly reduced in costs while improving accuracy as pioneered by Jim Otvos and associates) results in a 22-25% reduction in cardiovascular events within one year, contrary to the longstanding claims by many in the medical industry that the superiority over existing methods was weak, even by statements of some proponents.
Since the later 1990s, because of the development of NMR measurements, it has been possible to clinically measure lipoprotein particles at lower cost [under $80 US (including shipping) & is decreasing; versus the previous costs of >$400 to >$5,000] and higher accuracy. There are two other assays for LDL-particles, however, like LDL-C, most only estimate LDL particle concentrations.
Direct LDL particle measurement by NMR was mentioned by the ADA and ACC, in a 28 March 2008 joint consensus statement, as having advantages for predicting individual risk of atherosclerosis disease events, but the statement noted that the test is less widely available, is more expensive [about $13.00 US (2015 without insurance coverage) from some labs which use the Vantera Analyzer]. Debate continues that it is "...unclear whether LDL particle size measurements add value to measurement of LDL-particle concentration", though outcomes have always tracked LDL-particle, not LDL-C, concentrations.
Using NMR, as pioneered by researcher Jim Otvos and the North Carolina State University academic research spin-off company LipoScience, the total LDL particle concentrations, in nmol/L plasma, are typically subdivided by percentiles referenced to the 5,382 men and women, not on any lipid medications, who are participating in the MESA trial.
Optimal ranges
The LDL particle concentrations are typically categorized by percentiles, <20%, 20–50%, 50th–80th%, 80th–95% and >95% groups of the people participating and being tracked in the MESA trial, a medical research study sponsored by the United States National Heart, Lung, and Blood Institute.
The lowest incidence of atherosclerotic events over time occurs within the <20% group, with increased rates for the higher groups. Multiple other measures, including particle sizes, small LDL particle concentrations, large total and HDL particle concentrations, along with estimations of insulin resistance pattern and standard cholesterol lipid measurements (for comparison of the plasma data with the estimation methods discussed above) are also routinely provided.
Lowering LDL-cholesterol
The mevalonate pathway serves as the basis for the biosynthesis of many molecules, including cholesterol. The enzyme 3-hydroxy-3-methylglutaryl coenzyme A reductase (HMG CoA reductase) is an essential component and performs the first of 37 steps within the cholesterol production pathway, and present in every animal cell.
Keep in mind that LDL-C is not a measurement of actual LDL particles; LDL-C is only an estimate (not measured from the individual's blood sample) of how much cholesterol is being transported by all LDL particles; either a smaller concentration of large particles or a high concentration of small particles. Also keep in mind that LDL particles carry many fat molecules (typically 3,000 to 6,000 fat molecules per LDL particle); this includes cholesterol, triglycerides, phospholipids and others. Thus even if the hundreds to thousands of cholesterol molecules within an average LDL particle were measured, this does not reflect the other fat molecules or even the number of LDL particles.
Pharmaceutical
Lifestyle
Antioxidants
Because LDL particles appear harmless until they are within the blood vessel walls and oxidized by free radicals, it has been postulated that ingesting antioxidants and minimizing free radical exposure may reduce LDL's contribution to atherosclerosis, though results are not conclusive.