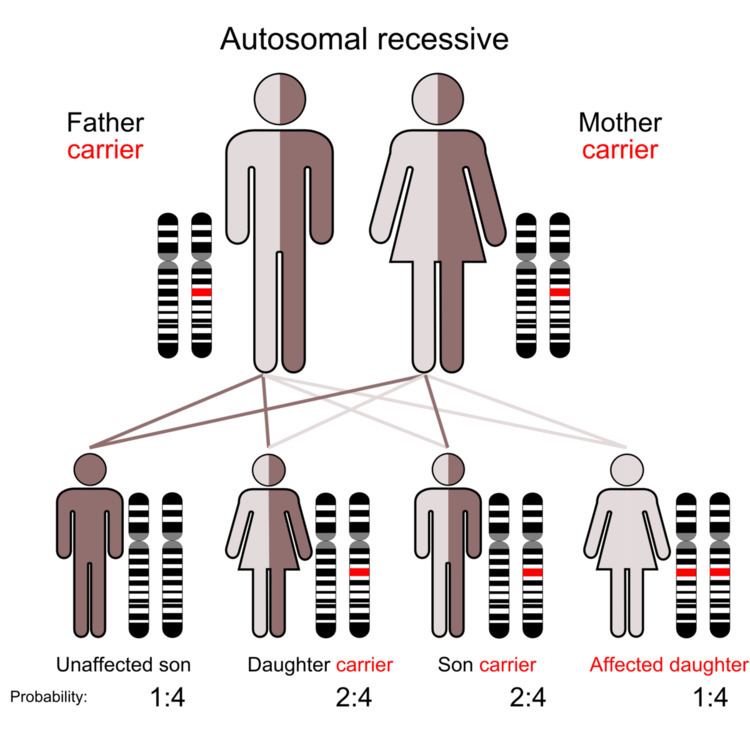
Idiopathic Infantile Arterial Calcification (IIAC) also known as Arterial Calcification of Infancy, Generalised Infantile Arterial Calcification (GACI), Idiopathic Arterial Calcification of Infancy (IACI), Occlusive Infantile Arterial Calcification, Occlusive Infantile Arteriopathy is an extremely rare, usually fatal genetic disorder, caused by mutations in the ENPP1 gene in 75% of the subjects. The condition affects infants during the first 6 months of life. This condition is inherited as an autosomal recessive pattern. It is characterized by generalised calcification of the arterial internal elastic lamina, leading to rupture of the lamina and occlusive changes in the tunica intima with stenosis and decreased elasticity of the vessel wall. Most infants die of vaso-occlusive disease, especially of the coronary arteries.
Clinical presentation is variable. First symptoms usually occur at birth but can take place in the first 6 months of life or in utero.
Decreased fetal activityGestation with an antenatal diagnosis of hydrops fetalisPolyhydramniosLow biophysical profileMarked cyanosisEdemaSevere hypertensionNo or fade pulsesRefusal of feedsTachypneaVomitingAbdominal distensionGeneral arterial rigidityCardiac failure (most common clinical finding)Strain patternThe disease results from an inactivating mutation in the ecto-nucleotide pyrophosphatase/phosphodiesterase-1 ENPP1 gene, leading to decreased inorganic pyrophosphate (PPi), a potent inhibitor of calcium deposition in the vessel wall. This mutation allows for unregulated calcium deposition within muscular arteries. The symptoms are caused by calcification of large and medium-sized arteries, including the aorta, coronary arteries, and renal arteries. Most of the patients die by 6 months of age because of heart failure. Recently, homozygous or compound heterozygous mutations for ENPP1 gene were reported as causative for the disorder. ENPP1 regulates extracellular inorganic pyrophosphate (PPi), a major inhibiter of extracellular matrix calcification.
Idiopathic arterial calcification of infancy should always be considered in infants and children presenting with hypertension, cardiac failure, or sudden death. Plain radiography, sonography and MRI can aid in the diagnosis. Postnatal gray-scale and color Doppler echocardiographic and sonographic examinations allowed noninvasive diagnosis, assessment of severity, and monitoring of progression. Contrast-enhanced MR angiography with breath-hold and cardiac gating techniques can allow evaluation of the extent of the disease.
Dilated and hypertrophied ventriclesExtramedullary hematopoiesis of liver Hypertrophy of myocardiumBright and hyper-reflective myocardiumPeriarticular calcifications in the wrists, ears, shoulders, ankles and hipHeart usually looks structurally normalCardiomegaly and pulmonary plethoraDiffuse arterial calcification involving aorta, carotid, cerebral, renal, mesenteric and cardiac arteriesEcho-dense aortic annulus, ascending aorta, transverse arch, descending aorta, main pulmonary artery, and coronary arteries unusually.Abdominal ultrasound can reveal hepatosplenomegaly, ascites, renal echogenicity and diffused arterial calcifications involving the aorta, common iliac, splenic, and renal arteries, as well as peritoneal calcifications involving the visceral peritoneum overlying the liver and intestineBrain ultrasound can show dilated lateral ventricles, poorly developed corpus callosum, and leukomalaciaEchocardiogram can reveal a structurally normal heart, normal ventricular function, however mild concentric ventricular hypertrophy and multiple intracardiac as well as vascular calcificationsIdiopathic arterial calcification of infancy should be suspected when there is hyperechogenicity of vessel walls, evidence of polyhydramnios or a past history of early neonatal deaths.DNA testing can identify one of the mutations responsible for the conditionPrevention and early detection
Potential role of genetic markers in the identification of persons at risk. There is a 75% probability to identify the two EPPN1 mutations (one paternal, one maternal) that cause IIAC. Once the mutations are identified, preimplantation genetic diagnosis (PGD) or chorionic villus sampling (CVS) are possible options to identify the condition, either before or during pregnancy.At week 20 of gestation, it is possible to detect an Echogenic intracardiac focus (EIF) or intravascular calcifications, particularly in the iliac and [abdominal aorta]. EIF is a small bright spot seen in the baby’s heart on an ultrasound exam. This is thought to represent mineralization, or small deposits of calcium hydroxyapatite, in the muscle of the heart. EIFs are found in about 3-5% of normal pregnancies and cause no health problems.Ultrasound can show subtle intravascular calcifications, particularly in the abdominal aorta at week 23.Calcification has been detected at 33 weeks' gestation.Prenatal and postnatal treatment with low-dose, cyclical bisphosphonates, also called diphosphonate, resulted in a complete resolution of vascular calcifications in some cases using disodium pamidronate and risedronate.PGE1 infusion is a possible therapeutic alternative for babies with idiopathic arterial calcification complicated by severe hypertension refractory to conventional treatment.Infants must reach a certain weight to allow for a transplant, commonly not reached.Although survival to adulthood has been reported, sometimes with persistent hypertension and cardiovascular sequelae, most patients die within the first 6 months of life.Spontaneous regression of arterial calcifications can occur, and antihypertensive treatment can be tapered off gradually. In some patients, the natural course of GACI may be more favourable than previously assumed.Despite the same genotype and similar sonographic and radiographic features in early infancy, the phenotype of IIAC can vary to a great extent within one family.