
 | ||
Hypertrophic cardiomyopathy, or HCM, is the leading cause of sudden cardiac death (SCD) in young athletes. HCM is frequently asymptomatic until SCD, and thus its prevention requires screening. Screening by medical history and physical exam are mostly ineffective, indicating heart abnormalities in only 3% of patients who subsequently suffered SCD. However, HCM can be detected with 80%+ accuracy by echocardiogram (ECHO), which may be combined with pre-screening by electrocardiogram (ECG). Routine cardiac screening of athletes has been implemented in Italy since 1982, and has resulted in an 89% drop in the incidence of SCD among screened athletes, from an unusually high starting rate. In the United States, citing cost concerns and low incidence, the American Heart Association has consistently opposed such routine screening. For rare conditions like HCM, the rate of false positive testing is also a significant concern. However, certain chapters of the American College of Cardiology are backing screening models provided by private entities and nonprofit organizations. Screen-positive individuals who are conclusively diagnosed with cardiac disease are usually told to avoid competitive athletics.
Contents
Description
HCM is a genetic disorder that causes the muscle of the heart (the myocardium) to thicken (or hypertrophy) without any apparent reason. When the heart thickens and becomes enlarged, particularly at the septum and left ventricle, it can cause dangerous arrhythmias (abnormal heart rhythms). The thickening of the heart also makes it harder for blood to leave, forcing the heart to work more vigorously to pump blood.
HCM occurs in approximately 2 per 1,000 people in the general population, being a primary and familial malformation. While younger individuals are likely to have a more severe form of hypertrophic cardiomyopathy, the condition is seen in people of all ages. Studies have shown that HCM is the most common cause of sudden cardiac death in athletes, accounting for approximately one-third of cases. Almost half of these HCM deaths happen during or just after physical exertion. The disease is equally prevalent in males and females, but 90% of HCM deaths in athletes occur in males, potentially due to their higher frequency of participation at a higher intensity. 60% of athletes are of high-school age at the time of death.
The first symptom of HCM among very young patients tends to be sudden collapse and possible death. However, other symptoms include exertional dyspnea (shortness of breath, most common), chest pain, dizziness, fainting, high blood pressure (hypertension), heart palpitations, and fatigue. Most young patients have no symptoms and may not realize they have the condition until it is found during a medical exam.
"Athlete's heart" versus HCM
Quite often, HCM can be mistaken for a condition known as "athlete's heart". Both involve thickening of the myocardium. However, athlete's heart generally is not correlated with SCD. While HCM can be linked to family history, athlete's heart arises purely as a function of intense exercise (usually at least an hour every day). Since the body is operating at high training levels, the heart adapts and grows in order to pump blood more efficiently. Stoppage of exercise for three months generally leads to a decrease in wall/septum thickness in those with athlete’s heart, whereas those with HCM exhibit no decline.
People with athlete's heart do not exhibit an abnormally enlarged septum, and the growth of heart muscle at the septum and free ventricular wall is symmetrical. The asymmetrical growth seen in HCM results in a less-dilated left ventricle. This in turn leads to a smaller volume of blood leaving the heart with each beat.
Screening and diagnosis
Screening young athletes to detect HCM is an important process in preventing a possible sudden cardiac death, as most victims do not show prior symptoms, and genetic testing is expensive and often inconclusive. Rarely, HCM can induce symptoms like dyspnea (difficulty breathing) or chest pain. However, other effects like myocarditis (an inflammation of the heart muscle) will likely be asymptomatic, and those at risk would only know if screened and diagnosed by a medical doctor.
There are three common methods of screening for HCM and sudden cardiac death, each with their own benefits and weaknesses:
1) Physical Examination and Medical History
Defined: Refers to a thorough but general physical examination that most patients or athletes would receive at any check-up with their doctor.
This method of screening, used for most young athletes in the United States, looks for some of the symptoms mentioned above, as well as heart palpitations or unusual chest X-rays. In addition, the existence of diseased family members that may have experienced sudden cardiac death is important because of the genetic transfer of the disease.
While cheap and easily performed by trained medical staff (doctors, physician assistants, nurse practitioners, registered nurses, paramedics, EMTs, trained medical and nursing students, and certain other medical and allied health professionals and paraprofessionals), it is impossible for a physical examination and medical history screening to identify the disease HCM.
2) 12-Lead Electrocardiogram (ECG)
Defined: Is a test performed by a doctor or trained health professional to measure the electrical signals produced by the heart.
The ECG cannot detect HCM directly, but is useful in detecting general heart abnormalities to recommend further testing, such as echocardiography. Even an asymptomatic HCM patient will demonstrate an abnormal ECG in 70% of cases. Although extra costs are associated with the equipment and professional assistance, it is an effective method of screening when used as a referral for echocardiography screening. The advantages: it is a relatively cheap and non-invasive, somewhat routine cardiovascular test that can be performed by a variety of persons with the requisite training, which just requires knowledge of cardiac anatomy and physiology and pathology, basic first aid, the cardiac cycle and electrical conduction (normal rhythm), abnormal rhythms (arrhythmias), the machine and proper lead placement (which are not extremely complicated and are taught early to many health students, using simpler versions, in a lab). There is some support for using a physical examination and ECG as a baseline screening for athletes, as a means to refer abnormal cases for definitive diagnoses of problems and to clear those with normal results. However, insurance may not cover such screening; sometimes, schools have organizations or groups of health students or professionals conduct them on a discounted or pro bono basis.
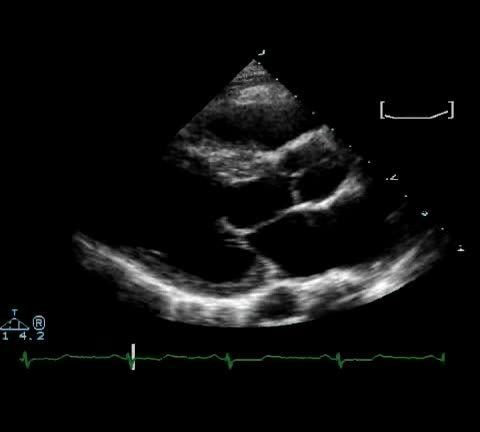
3) Echocardiography (ECHO)
Defined: A Transthoracic Echocardiogram provides a 2-D image to a doctor from standard ultrasound that is directly and reliably able to detect HCM in athletes.
This procedure is expensive but is considered to be optimally used when implemented after an abnormal ECG, and is the only test of choice to confirm an HCM diagnosis. Studies indicate that doctors are able to detect HCM from an ECHO at least 80% of the time.
A full ECHO may cost $400–$1,000 in the United States, but a targeted ECHO for HCM screening may be performed in 2.5 minutes at a cost of $35, as is done by Purdue University.
Italy
By law, all competitive athletes are required to undergo physiological testing prior to competing. This consists of a history, physical examination, urinalysis, resting and exercise ECG, and pulmonary functioning test. All of these are conducted by a sports physician. If there are abnormalities, further screening by ECHO (echocardiography) is required.
European Association for Cardiovascular Prevention
This is supported by the International Olympic Committee, and follows the Italian strategy, with personal and family history, physical examination, and 12-lead resting ECG. FIFA also required cardiac screening of all soccer players in the 2006 World Cup tournament in Germany.
United States
As of 2014, there was no national policy for the screening of cardiovascular disease in young athletes, though many screening programs were being run by private entities and various nonprofit organizations. Most state laws require competitive athletes to undergo a physician-mediated physical examination and history. A medical history and physical examination were found to have little sensitivity or power to detect HCM; but ECG or echocardiograms are rarely used, due to the low incidence of HCM, approximately 2 in 1,000 individuals.