
Specialty emergency medicine ICD-9-CM 673.8, 958.1 eMedicine med/652 | ICD-10 O88.8, T79.1 DiseasesDB 4766 MeSH D004620 | |
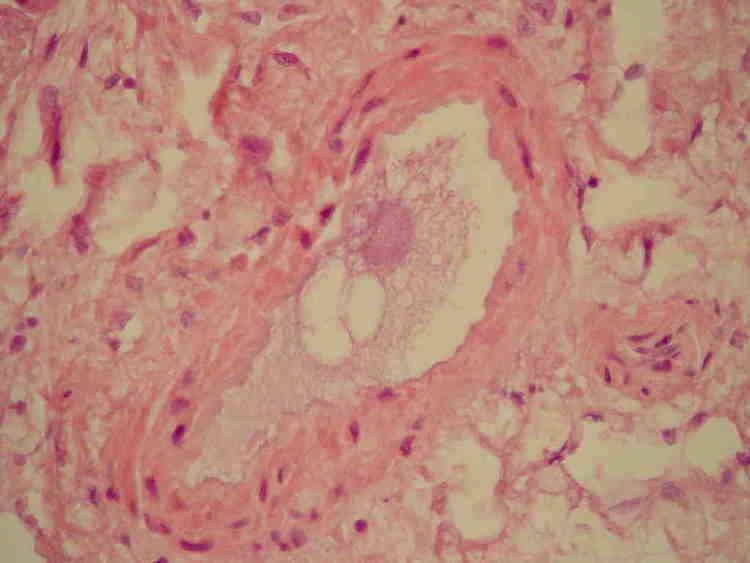 | ||
A fat embolism is a type of embolism in which the embolus consists of fatty material. They are often caused by physical trauma such as fracture of long bones, soft tissue trauma, and burns.
Contents
Signs and symptoms
An asymptomatic latent period of about 12–48 hours precedes the clinical signs and symptoms. The severe form presents as acute pulmonary heart disease and respiratory failure. This may lead to death within a few hours of injury.
Clinical fat embolism syndrome presents with tachycardia, tachypnea, elevated temperature, hypoxemia, hypercapnia, thrombocytopenia, and occasionally mild neurological symptoms.
A petechial rash also called purpura that appears on the upper anterior portion of the body, including the chest, neck, upper arm, axilla, shoulder, oral mucosa and conjunctivae is considered to be a pathognomonic sign of Fat embolism syndrome (FES), however, it appears late and often disappears within hours. It results from occlusion of dermal capillaries by fat, and increased capillary fragility.
Central nervous system (CNS) signs, including a change in level of consciousness, are not uncommon. They are usually nonspecific and have the features of diffuse encephalopathy: acute confusion, stupor, coma, rigidity (neurology), or convulsions. Cerebral edema contributes to the neurologic deterioration.
Unlike emboli that arise from blood clots, fat emboli are small and multiple, and thus have widespread effects.
FES is distinct from the presence of fat emboli. Symptoms usually occur 1–3 days after a traumatic injury and are predominantly pulmonary (shortness of breath, hypoxemia), neurological (agitation, delirium, or coma), dermatological (petechial rash), and haematological (anaemia, low platelets). The syndrome manifests more frequently in closed fractures of the pelvis or long bones. The petechial rash, which usually resolves in 5–7 days, is said to be pathognomonic for the syndrome, but only occurs in 20–50% of cases.
Cause
Fat emboli occur in almost 90% of all people with severe injuries to bones, although only 10% of these are symptomatic. The risk of fat embolism syndrome is thought to be reduced by early immobilization of fractures and especially by early operative correction. There is also some evidence that steroid prophylaxis of high-risk patients reduces the incidence. The mortality rate of fat-embolism syndrome is approximately 10–20%.
Fat emboli can be either traumatic (resulting from fracture of long bones, accidents, or trauma to soft tissue) or non-traumatic (resulting from burns or fatty liver).
Pathogenesis
The pathogenesis occurs due to both mechanical obstruction and biochemical injury. It is aggravated by local platelet and erythrocyte aggregation. The release of fatty acids from the fat globules also causes local toxic injury to endothelium. The vascular damage is aggravated by platelet activation and recruitment of granulocytes.
Several mechanisms have been proposed to explain the pathogenesis of fat embolism. They may be acting together or singly.
- Mechanical. Mobilisation of fluid fat following trauma to bone and soft tissue.
- Emulsion instability. Explains the pathogenesis of fat embolism in non-traumatic cases. Fat embolus formed by aggregation of plasma lipids (chylomicrons and fatty acids) due to disturbances in emulsification of fat. Symptoms include fatty liver (hepatic steatosis).
- Intravascular coagulation. May result from disseminated intravascular coagulation (DIC).
- Toxic injury. Blood vessels injured by high plasma levels of free fatty acid, results in increased vascular permeability and consequently pulmonary edema.
Complications
Complications from a fat embolism tend to be serious:
- Pulmonary fat embolism. Widespread obstruction causes sudden death.
- Systemic fat embolism. These may get lodged in capillaries of organs like brain, kidney, skin etc., causing minute hemorrhage and microinfarcts.
Embolized fat travels through the venous system to the lungs and can occlude pulmonary capillaries. Fat emboli may cause cor pulmonale if adequate compensatory pulmonary vasodilation does not occur.
Circulating free fatty acids are directly toxic to pneumocytes and capillary endothelium in the lung, causing interstitial hemorrhage, edema and chemical pneumonitis.
Diagnosis
Diagnosis of FES may be difficult because, except for the petechiae, there are no pathognomonic signs. Laboratory tests are mostly nonspecific:
The chest X-ray may show evenly distributed, fleck-like pulmonary shadows (snow storm appearance), increased pulmonary markings and enlargement of the right side of the heart.
Hypoxemia is present in nearly all patients with FES, often to a PaO2 of well below 60 mmHg. Arterial hypoxemia in these patients has been attributed to ventilation-perfusion inequality and intrapulmonary shunting. Acute cor pulmonale is manifested by respiratory distress, hypoxemia, hypotension and elevated central venous pressure.
Treatment
The most effective prophylactic measure is to reduce long bone fractures as soon as possible after the injury.
Maintenance of intravascular volume is important because shock can exacerbate the lung injury caused by FES. Albumin has been recommended for volume resuscitation in addition to balanced electrolyte solution, because it not only restores blood volume but also binds fatty acids, and may decrease the extent of lung injury.