
ICD-9-CM 337.9 | ICD-10 G90 MeSH D001342 | |
 | ||
Dysautonomia is a term for a group of diseases that include postural orthostatic tachycardia syndrome (POTS), multiple system atrophy, autonomic failure, and autonomic neuropathy. In these conditions the autonomic nervous system (ANS) does not work properly. Dysautonomia is most often a type of neuropathy affecting the nerves that carry information from the brain and spinal cord to the heart, bladder, intestines, sweat glands, pupils, and blood vessels; although it has many causes, not all of which classify as neuropathic.
Contents
The diagnosis is achieved through functional testing of the autonomic nervous system, focusing on the organ system affected. Investigations may be performed to identify underlying disease processes that may have led to the development of symptoms or autonomic neuropathy. Symptomatic treatment is available for many symptoms associated with dysautonomia, and some disease processes can be treated directly.
Signs and symptoms
The symptoms of dysautonomia are numerous and vary widely for each individual,symptoms of dysautonomia are due to inefficient or unbalanced efferent signals sent via both systems. The primary symptoms present in individuals with dysautonomia include:
Causes
Dysautonomia may be due to inherited or degenerative neurologic diseases (primary dysautonomia) or it may occur due to injury of the autonomic nervous system from an acquired disorder (secondary dysautonomia). The most common causes of dysautonomia include:
In the sympathetic nervous system predominant dysautonomia is common along with fibromyalgia, chronic fatigue syndrome, irritable bowel syndrome, and interstitial cystitis, raising the possibility that such dysautonomia could be their common clustering underlying pathogenesis.
Mechanism
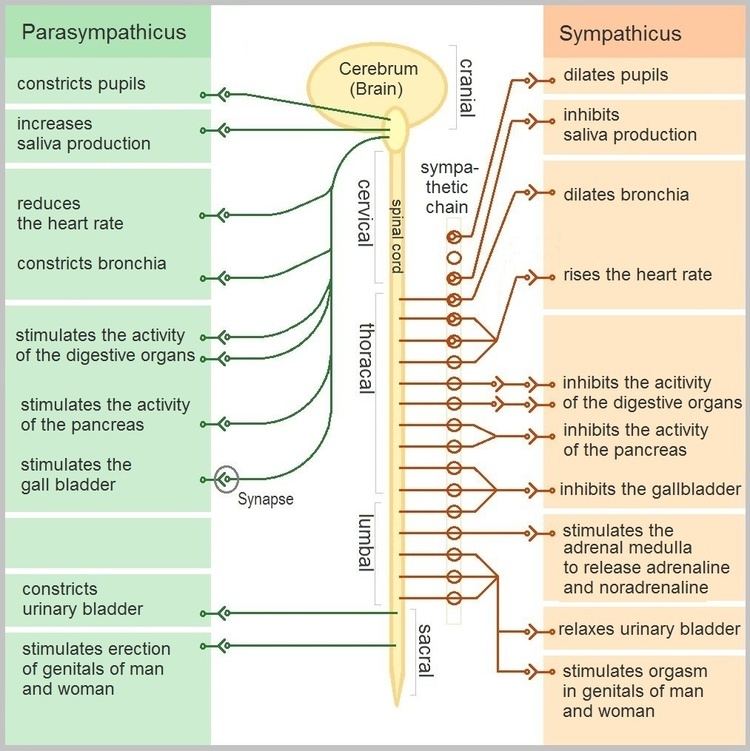
The autonomic nervous system (ANS) is a component of the peripheral nervous system and is made up of two branches: the sympathetic nervous system (SNS) and the parasympathetic nervous system (PNS). The SNS controls the more active responses such as increasing heart rate and blood pressure. The PNS slows down the heart rate and aids in digestion,for example. Symptoms typically arise from abnormal responses of either the sympathetic or parasympathetic systems based on situation or environment.
Diagnosis
The diagnosis of dysautonomia depends on the overall function of three autonomic functions - cardiovagal, adrenergic, and sudomotor. A diagnosis should, at a bare minimum, include measurements of blood pressure and heart rate while lying flat, and after at least 3 minutes of standing. The best way to achieve a diagnosis includes a range of testing, notably an autonomic reflex screen, tilt table test, and testing of the sudomotor response (QSART or thermoregulatory sweat test). Additional tests and exams to determine a diagnosis of dysautonomia include the following:
Management
The treatment of dysautonomia can be difficult, since it is made up of many different symptoms, a combination of drug therapies is often required to manage individual symptomatic complaints. Therefore, if an autoimmune neuropathy is the case, then treatment with immunomodulatory therapies is done, or if diabetes mellitus is the cause, control of blood glucose is important. In treatment there can be: proton-pump inhibitors and H2 receptor antagonists used for digestive symptoms such as acid reflux.
For the treatment of genitourinary autonomic neuropathy medications may include sildenafil (a guanine monophosphate type-5 phosphodiesterase inhibitor). For the treatment of hyperhidrosis, anticholinergic agents such as trihexyphenidyl or scopolamine can be used, also intracutaneous injection of botulinum toxin type A can be used for management in some cases.
Prognosis
The prognosis of dysautonomia depends on several factors, individuals with chronic, progressive, generalized dysautonomia in the setting of central nervous system degeneration such as Parkinson's disease or multiple system atrophy have a generally poorer long-term prognosis. Consequently, dysautonomia could be fatal due to pneumonia, acute respiratory failure, or sudden cardiopulmonary arrest.
According to Vinik, et al., it was found that autonomic dysfunction symptoms such as orthostatic hypotension, gastroparesis, and gustatory sweating are more frequently identified in mortalities.