
Specialty medical genetics ICD-9-CM 756.0 DiseasesDB 3203 | ICD-10 Q75.1 OMIM 123500 eMedicine ped/511 derm/734 | |
 | ||
Crouzon syndrome is an autosomal dominant genetic disorder known as a branchial arch syndrome. Specifically, this syndrome affects the first branchial (or pharyngeal) arch, which is the precursor of the maxilla and mandible. Since the branchial arches are important developmental features in a growing embryo, disturbances in their development create lasting and widespread effects.
Contents
This syndrome is named after Octave Crouzon, a French physician who first described this disorder. He noted the affected patients were a mother and her daughter, implying a genetic basis. First called "craniofacial dysostosis", the disorder was characterized by a number of clinical features. This syndrome is caused by a mutation in the fibroblast growth factor receptor II, located on chromosome 10.
Breaking down the name, "craniofacial" refers to the skull and face, and "dysostosis" refers to malformation of bone.
Now known as Crouzon syndrome, the characteristics can be described by the rudimentary meanings of its former name. What occurs is that an infant's skull and facial bones, while in development, fuse early or are unable to expand. Thus, normal bone growth cannot occur. Fusion of different sutures leads to different patterns of growth of the skull.
Examples include: trigonocephaly (fusion of the metopic suture), brachycephaly (fusion of the coronal suture), dolichocephaly (fusion of the sagittal suture), plagiocephaly (unilateral premature closure of lambdoid and coronal sutures), oxycephaly (fusion of coronal and lambdoidal sutures), Kleeblattschaedel (premature closure of all sutures).
Signs and symptoms
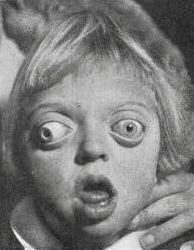
As a result of the changes to the developing embryo, the symptoms are very pronounced features, especially in the face. Low-set ears are a typical characteristic, as in all of the disorders which are called branchial arch syndromes. The reason for this abnormality is that ears on a foetus are much lower than those on an adult. During normal development, the ears "travel" upward on the head; however, in Crouzon patients, this pattern of development is disrupted. Ear canal malformations are extremely common, generally resulting in some hearing loss. In particularly severe cases, Ménière's disease may occur.
The most notable characteristic of Crouzon syndrome is craniosynostosis, as described above; however it usually presents as brachycephaly resulting in the appearance of a short and broad head. Exophthalmos (bulging eyes due to shallow eye sockets after early fusion of surrounding bones), hypertelorism (greater than normal distance between the eyes), and psittichorhina (beak-like nose) are also symptoms. Additionally, external strabismus is a common occurrence, which can be thought of as opposite from the eye position found in Down syndrome. Lastly, hypoplastic maxilla (insufficient growth of the midface) results in relative mandibular prognathism (chin appears to protrude despite normal growth of mandible) and gives the effect of the patient having a concave face. Crouzon syndrome is also associated with patent ductus arteriosus (PDA) and aortic coarctation.
For reasons that are not entirely clear, most Crouzon patients also have noticeably shorter humerus and femur bones relative to the rest of their bodies than members of the general population. A small percentage of Crouzon patients also have what is called "Type II" Crouzon syndrome, distinguished by partial syndactyly.
Causes
The current research indicates fibroblast growth factor receptors (FGFR) FGFR2 and FGFR3 as the leading factors in causing the autosomal dominant Crouzon Syndrome. These two transmembrane proteins are two of four fibroblast growth factor receptors involved in osteoblast differentiation during embryonic development; mutations amongst these receptors are involved in several genetic disorders. There are 40 known mutations, most of which are caused by a missense mutation. FGFR2 is the most commonly mutated gene, a missense at cysteine 342 in exon 9, which creates a gain-of-function. The FGFR2lllc isoform, created via alternative splicing of exon 3 of the FGFR2 gene, uses exon 9 and is used in mesenchymal stem cells to control ossification. However, the mutation constitutively activates the transmembrane protein via a disulfide bond formed incorrectly due to the loss of cysteine 342. FGFR3 is expressed more in the frontal bones during embryonic development, guiding cranial bone development. A point mutation causes constitutive activation of tyrosine in the activation loop, located in the cytosolic region of the protein, leading to accelerated differentiation of frontal osteoblasts. Resulting in premature fusion of frontal cranial bones.
Diagnosis
Diagnosis of Crouzon syndrome usually can occur at birth by assessing the signs and symptoms of the baby. Further analysis, including radiographs, magnetic resonance imaging (MRI) scans, genetic testing, X-rays and CT scans can be used to confirm the diagnosis of Crouzon syndrome.
Treatment
Each child is different and it entirely depends on which sutures are fused and how it is affecting the child as to how it is treated. Some children have severe breathing issues due to shallow mid face and may require a tracheostomy. All should be treated at a specialist centre. Cranio bands are not used in the UK.
Surgery is typically used to prevent the closure of sutures of the skull from damaging the brain's development. Without surgery, blindness and mental retardation are typical outcomes. Craniofacial surgery is a discipline of both plastic surgery and Oral and maxillofacial surgery (OMS) . To move the orbits forward, craniofacial surgeons expose the skull and orbits and reshape the bone. To treat the midface deficiency, craniofacial surgeons can move the lower orbit and midface bones forward. For jaw surgery, either plastic surgeons or oral and maxillofacial (OMFS) surgeons can perform these operations.
Crouzon patients tend to have multiple sutures involved, most specifically bilateral coronal craniosynostoses, and either open vault surgery or strip craniectomy (if child is under 6 months) can be performed. In the later scenario, a helmet is worn for several months following surgery.
Once treated for the cranial vault symptoms, Crouzon patients generally go on to live a normal lifespan.
Epidemiology
Incidence of Crouzon syndrome is currently estimated to occur in 1.6 out of every 100,000 people. There is a greater frequency in families with a history of the disorder, but that doesn't mean that everyone in the family is affected (as referred to above).
Dental significance
For dentists, this disorder is important to understand since many of the physical abnormalities are present in the head, and particularly the oral cavity. Common features are a narrow/high-arched palate, posterior bilateral crossbite, hypodontia (missing some teeth), and crowding of teeth. Due to maxillary hypoplasia,
Crouzon patients generally have a considerable permanent underbite and subsequently cannot chew using their incisors. For this reason, people with Crouzon syndrome sometimes eat in an unusual way—eating chicken drumsticks with a fork, for example, or breaking off pieces of a sandwich rather than taking a bite into it.