
Product name Cannabis Geographic origin Central and South Asia | Part(s) of plant flower | |
 | ||
Main producers Afghanistan, Canada, China, Colombia, India, Jamaica, Lebanon, Mexico, Morocco, Netherlands, Pakistan, Paraguay, Spain, Thailand, Turkey, United States | ||
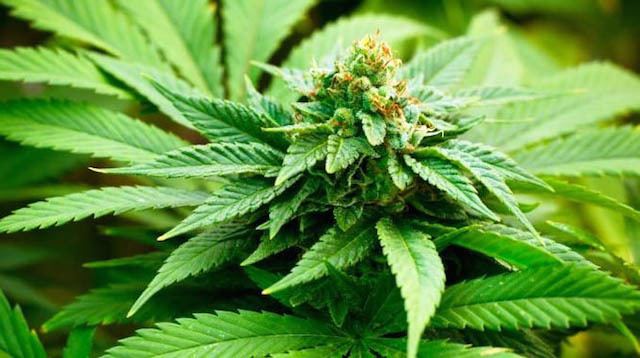
Cannabis, also known as marijuana among several other names, is a preparation of the Cannabis plant intended for use as a psychoactive drug or medicine. The main psychoactive part of cannabis is tetrahydrocannabinol (THC); one of 483 known compounds in the plant, including at least 65 other cannabinoids. Cannabis can be used by smoking, vaporization, within food, or as an extract.
Contents
- Medical
- Recreational
- Spiritual
- Available forms
- Adverse effects
- Toxicity
- Lungs
- Cancer
- Cardiovascular
- Neurological
- Psychiatric
- Chronic use
- Tolerance and withdrawal
- Motor vehicle crashes
- Mechanism of action
- Detection in body fluids
- Varieties and strains
- Psychoactive ingredients
- Marijuana
- Kief
- Hashish
- Tincture
- Hash oil
- Infusions
- Adulterated cannabis
- Medical use
- History
- Legal status
- Usage
- United States
- Production
- Price
- Distribution
- Gateway drug
- Research
- References

Cannabis is often used for its mental and physical effects, such as a "high" or "stoned" feeling, a general change in perception, euphoria (heightened mood), and an increase in appetite. Short term side effects may include a decrease in short-term memory, dry mouth, impaired motor skills, red eyes, and feelings of paranoia or anxiety. Long term side effects may include addiction, decreased mental ability in those who started as teenagers, and behavioral problems in children whose mothers used cannabis during pregnancy. Onset of effects is within minutes when smoked and about 30 to 60 minutes when cooked and eaten. They last for between two and six hours.

Cannabis is mostly used recreationally or as a medicinal drug. It may also be used for religious or spiritual purposes. In 2013, between 128 and 232 million people used cannabis (2.7% to 4.9% of the global population between the ages of 15 and 65). In 2015, 43% of Americans had used cannabis, which increased to 51% in 2016. About 12% have used it in the past year, and 7.3% have used it in the past month. This makes it the most commonly used illegal drug both in the world and the United States.

The earliest recorded uses date from the 3rd millennium BC. Since the early 20th century, cannabis has been subject to legal restrictions. The possession, use, and sale of cannabis is illegal in most countries of the world. Medical cannabis refers to the physician-recommended use of cannabis, which is taking place in Canada, Belgium, Australia, the Netherlands, Spain, and 23 U.S. states. Cannabis use started to become popular in the US in the 1970s. Support for legalization has increased in the United States and several US states have legalized recreational or medical use.
Medical

Medical cannabis, or medical marijuana can refer to the use of cannabis and its cannabinoids to treat disease or improve symptoms; however, there is no single agreed upon definition. The use of cannabis as a medicine has not been rigorously scientifically tested, often due to production restrictions and other federal regulations. There is limited evidence suggesting cannabis can be used to reduce nausea and vomiting during chemotherapy, to improve appetite in people with HIV/AIDS, and to treat chronic pain and muscle spasms. Its use for other medical applications is insufficient for conclusions about safety or efficacy.

Short-term use increases the risk of both minor and major adverse effects. Common side effects include dizziness, feeling tired, vomiting, and hallucinations. Long-term effects of cannabis are not clear. Concerns include memory and cognition problems, risk of addiction, schizophrenia in young people, and the risk of children taking it by accident.
Recreational

Cannabis has psychoactive and physiological effects when consumed. The immediate desired effects from consuming cannabis include relaxation and euphoria (the "high" or "stoned" feeling), a general alteration of conscious perception, increased awareness of sensation, increased libido and distortions in the perception of time and space. At higher doses, effects can include altered body image, auditory and/or visual illusions, pseudohallucinations and ataxia from selective impairment of polysynaptic reflexes. In some cases, cannabis can lead to dissociative states such as depersonalization and derealization.

Some immediate undesired side effects include a decrease in short-term memory, dry mouth, impaired motor skills and reddening of the eyes. Aside from a subjective change in perception and mood, the most common short-term physical and neurological effects include increased heart rate, increased appetite and consumption of food, lowered blood pressure, impairment of short-term and working memory, psychomotor coordination, and concentration. Some users may experience an episode of acute psychosis, which usually abates after six hours, but in rare instances, heavy users may find the symptoms continuing for many days. A reduced quality of life is associated with heavy cannabis use, although the relationship is weaker than for tobacco and other substances.
Spiritual

Cannabis has held sacred status in several religions. It has been used in an entheogenic context – a chemical substance used in a religious, shamanic, or spiritual context - in India and Nepal since the Vedic period dating back to approximately 1500 BCE, but perhaps as far back as 2000 BCE. There are several references in Greek mythology to a powerful drug that eliminated anguish and sorrow. Herodotus wrote about early ceremonial practices by the Scythians, thought to have occurred from the 5th to 2nd century BCE. In modern culture the spiritual use of cannabis has been spread by the disciples of the Rastafari movement who use cannabis as a sacrament and as an aid to meditation. The earliest known reports regarding the sacred status of cannabis in India and Nepal come from the Atharva Veda estimated to have been written sometime around 2000–1400 BCE.
Available forms
Cannabis is consumed in many different ways:

Adverse effects
According to the United States Department of Health and Human Services, there were 455,000 emergency room visits associated with cannabis use in 2011. These statistics include visits in which the patient was treated for a condition induced by or related to recent cannabis use. The drug use must be "implicated" in the emergency department visit, but does not need to be the direct cause of the visit. Most of the illicit drug emergency room visits involved multiple drugs. In 129,000 cases, cannabis was the only implicated drug.
Heavy, long term exposure to marijuana may have biologically-based physical, mental, behavioral and social health consequences and may be "associated with diseases of the liver (particularly with co-existing hepatitis C), lungs, heart, and vasculature". It is recommended that cannabis use be stopped before and during pregnancy as it can result in negative outcomes for both the mother and baby. However, maternal use of marijuana during pregnancy does not appear to be associated with low birth weight or early delivery after controlling for tobacco use and other confounding factors. A 2014 review found that while cannabis use may be less harmful than alcohol use, the recommendation to substitute it for problematic drinking is premature without further study.
Toxicity
THC, the principal psychoactive constituent of the cannabis plant, has low toxicity. The dose of THC needed to kill 50% of tested rodents is extremely high. Acute effects may include anxiety and panic, impaired attention, and memory (while intoxicated), an increased risk of psychotic symptoms, and possibly an increased risk of accidents if a person drives a motor vehicle while intoxicated. Short-term cannabis intoxication can hinder the mental processes of organizing and collecting thoughts. This condition is known as temporal disintegration. Psychotic episodes are well-documented and typically resolve within minutes or hours. There have been few reports of symptoms lasting longer. Cannabis has not been reported to cause fatal overdose. Studies have found that cannabis use during adolescence is associated with impairments in memory that persist beyond short-term intoxication.
Lungs
A limited number of studies have examined the effects of cannabis smoking on the respiratory system. Chronic heavy marijuana smoking is associated with coughing, production of sputum, wheezing, and other symptoms of chronic bronchitis. The available evidence does not support a causal relationship between cannabis use and chronic obstructive pulmonary disease. Short-term use of cannabis is associated with bronchodilation.
Cancer
Cannabis smoke contains thousands of organic and inorganic chemical compounds. This tar is chemically similar to that found in tobacco smoke, and over fifty known carcinogens have been identified in cannabis smoke, including; nitrosamines, reactive aldehydes, and polycylic hydrocarbons, including benz[a]pyrene. Cannabis smoke is also inhaled more deeply than is tobacco smoke. As of 2015, there is no consensus regarding whether cannabis smoking is associated with an increased risk of cancer. Light and moderate use of cannabis is not believed to increase risk of lung or upper airway cancer. Evidence for causing these cancers is mixed concerning heavy, long-term use. In general there are far lower risks of pulmonary complications for regular cannabis smokers when compared with those of tobacco. A 2015 review found an association between cannabis use and the development of testicular germ cell tumors (TGCTs), particularly non-seminoma TGCTs. A 2015 analysis of six studies found little evidence that long-term or regular cannabis smoking was associated with lung cancer risk, though it could not rule out whether an association with heavy smoking exists. Another 2015 meta-analysis found no association between lifetime cannabis use and risk of head or neck cancer. Combustion products are not present when using a vaporizer, consuming THC in pill form, or consuming cannabis foods.
Cardiovascular
There is serious suspicion among cardiologists, spurring research but falling short of definitive proof, that cannabis use has the potential to contribute to cardiovascular disease. Cannabis is believed to be an aggravating factor in rare cases of arteritis, a serious condition that in some cases leads to amputation. Because 97% of case-reports also smoked tobacco, a formal association with cannabis could not be made. If cannabis arteritis turns out to be a distinct clinical entity, it might be the consequence of vasoconstrictor activity observed from delta-8-THC and delta-9-THC. Other serious cardiovascular events including myocardial infarction, stroke, sudden cardiac death, and cardiomyopathy have been reported to be temporally associated with cannabis use. Research in these events is complicated because cannabis is often used in conjunction with tobacco, and drugs such as alcohol and cocaine. These putative effects can be taken in context of a wide range of cardiovascular phenomena regulated by the endocannabinoid system and an overall role of cannabis in causing decreased peripheral resistance and increased cardiac output, which potentially could pose a threat to those with cardiovascular disease. There is some evidence from case reports that cannabis use may provoke fatal cardiovascular events in young people who have not been diagnosed with cardiovascular disease. Smoking cannabis has also been shown to increase the risk of myocardial infarction by 4.8 times for the 60 minutes after consumption.
Neurological
Cannabis use is associated with neuroanatomic alterations in brain regions rich in cannabinoid receptors, such as the hippocampus, prefrontal cortex, amygdala, and cerebellum. The same review found that greater dose of marijuana and earlier age at onset of use were also associated with such alterations. A 2010 review found resting blood flow to be lower globally and in prefrontal areas of the brain in cannabis users, when compared to non-users. It was also shown that giving THC or cannabis correlated with increased bloodflow in these areas, and facilitated activation of the anterior cingulate cortex and frontal cortex when participants were presented with assignments demanding use of cognitive capacity. Both reviews noted that some of the studies that they examined had methodological limitations, for example small sample sizes or not distinguishing adequately between cannabis and alcohol consumption. Cannabis users appear to have smaller hippocampi than nonusers; this finding is based on a series of small studies with inconsistent designs, so it is uncertain. A 2016 meta-analysis found that regular cannabis users tended to have cue reactivity, the intensity of which ranged from moderate to very high.
There is limited evidence that chronic cannabis use can reduce levels of glutamate metabolites in the human brain.
A 2012 meta-analysis found that the effects of cannabis use on neurocognitive functions were "limited to the first 25 days of abstinence" and that there was no evidence that such use had long-lasting effects, while a 2011 review found that cannabis use impaired cognitive functions on several levels, ranging from basic coordination to executive function tasks.
Psychiatric
Epidemiological studies have found a strong correlation between cannabis use and the risk of psychosis, and found the risk is higher for with strains higher in THC. However, not all researchers consider this association to reflect a cause-and-effect relationship between cannabis use and psychosis.
It is not clear whether cannabis use affects the rate of suicide. It may increase the risk of depression, but further research is needed in this area.
Chronic use
Effects of chronic use may include bronchitis, a cannabis dependence syndrome, and subtle impairments of attention and memory. These deficits persist while chronically intoxicated. There is little evidence that cognitive impairments persist in adult abstinent cannabis users. Compared to non-smokers, people who smoked cannabis regularly in adolescence exhibit reduced connectivity in specific brain regions associated with memory, learning, alertness, and executive function. A study has suggested that sustained heavy, daily, adolescent onset cannabis use over decades is associated with a decline in IQ by age 38. No effects were found in those who initiated cannabis use later, or in those who ceased use earlier in adulthood.
Tolerance and withdrawal
Cannabis usually causes no tolerance or withdrawal symptoms except in heavy users. In a survey of heavy users, 42.4% experienced withdrawal symptoms when they tried to quit marijuana, such as craving, irritability, boredom, anxiety and sleep disturbances. About 9% of those who experiment with marijuana eventually become dependent. The rate goes up to 1 in 6 among those who begin use as adolescents, and one-quarter to one-half of those who use it daily according to a NIDA review. A 2013 review estimates daily use is associated with a 10-20% rate of dependence. The highest risk of cannabis dependence is found in those with a history of poor academic achievement, deviant behavior in childhood and adolescence, rebelliousness, poor parental relationships, or a parental history of drug and alcohol problems. Cannabis withdrawal is less severe than withdrawal from alcohol.
Motor vehicle crashes
Marijuana is the most common illegal drug reported in motor vehicle accidents. A 2012 meta-analysis found that cannabis use was associated with an increased risk of being involved in a motor vehicle crash. A 2016 review also found a statistically significant increase in crash risk associated with marijuana use, but noted that this risk was "of low to medium magnitude." The increase in risk of motor vehicle crash for cannabis use is between 2 and 3 times relative to baseline, whereas that for comparable doses of alcohol is between 6 and 15 times.
Mechanism of action
The high lipid-solubility of cannabinoids results in their persisting in the body for long periods of time. Even after a single administration of THC, detectable levels of THC can be found in the body for weeks or longer (depending on the amount administered and the sensitivity of the assessment method). A number of investigators have suggested that this is an important factor in marijuana's effects, perhaps because cannabinoids may accumulate in the body, particularly in the lipid membranes of neurons.
Not until the end of the 20th century was the specific mechanism of action of THC at the neuronal level studied. Researchers have subsequently confirmed that THC exerts its most prominent effects via its actions on two types of cannabinoid receptors, the CB1 receptor and the CB2 receptor, both of which are G-protein coupled receptors. The CB1 receptor is found primarily in the brain as well as in some peripheral tissues, and the CB2 receptor is found primarily in peripheral tissues, but is also expressed in neuroglial cells. THC appears to alter mood and cognition through its agonist actions on the CB1 receptors, which inhibit a secondary messenger system (adenylate cyclase) in a dose dependent manner. These actions can be blocked by the selective CB1 receptor antagonist SR141716A (rimonabant), which has been shown in clinical trials to be an effective treatment for smoking cessation, weight loss, and as a means of controlling or reducing metabolic syndrome risk factors. However, due to the dysphoric effect of CB1 antagonists, this drug is often discontinued due to these side effects.
Via CB1 activation, THC indirectly increases dopamine release and produces psychotropic effects. Cannabidiol also acts as an allosteric modulator of the mu and delta opioid receptors. THC also potentiates the effects of the glycine receptors. The role of these interactions in the "marijuana high" remains elusive.
Detection in body fluids
THC and its major (inactive) metabolite, THC-COOH, can be measured in blood, urine, hair, oral fluid or sweat using chromatographic techniques as part of a drug use testing program or a forensic investigation of a traffic or other criminal offense. The concentrations obtained from such analyses can often be helpful in distinguishing active use from passive exposure, elapsed time since use, and extent or duration of use. These tests cannot, however, distinguish authorized cannabis smoking for medical purposes from unauthorized recreational smoking. Commercial cannabinoid immunoassays, often employed as the initial screening method when testing physiological specimens for marijuana presence, have different degrees of cross-reactivity with THC and its metabolites. Urine contains predominantly THC-COOH, while hair, oral fluid and sweat contain primarily THC. Blood may contain both substances, with the relative amounts dependent on the recency and extent of usage.
The Duquenois–Levine test is commonly used as a screening test in the field, but it cannot definitively confirm the presence of cannabis, as a large range of substances have been shown to give false positives. Despite this, it is common in the United States for prosecutors to seek plea bargains on the basis of positive D–L tests, claiming them to be conclusive, or even to seek conviction without the use of gas chromatography confirmation, which can only be done in the lab. In 2011, researchers at John Jay College of Criminal Justice reported that dietary zinc supplements can mask the presence of THC and other drugs in urine. However, a 2013 study conducted by researchers at the University of Utah School of Medicine refute the possibility of self-administered zinc producing false-negative urine drug tests.
Varieties and strains
CBD is a 5-HT1A receptor agonist, which may also contribute to an anxiolytic effect. This likely means the high concentrations of CBD found in Cannabis indica mitigate the anxiogenic effect of THC significantly. The effects of sativa are well known for their cerebral high, hence its daytime use as medical cannabis, while indica is well known for its sedative effects and preferred night time use as medical cannabis.
Psychoactive ingredients
According to the United Nations Office on Drugs and Crime (UNODC), "the amount of THC present in a cannabis sample is generally used as a measure of cannabis potency." The three main forms of cannabis products are the flower, resin (hashish), and oil (hash oil). The UNODC states that cannabis often contains 5% THC content, resin "can contain up to 20% THC content", and that "Cannabis oil may contain more than 60% THC content."
A 2012 review found that the THC content in marijuana had increased worldwide from 1970 to 2009. It is unclear, however, whether the increase in THC content has caused people to consume more THC or if users adjust based on the potency of the cannabis. It is likely that the higher THC content allows people to ingest less tar. At the same time, Cannabidiol (CBD) levels in seized samples have lowered, in part because of the desire to produce higher THC levels and because more illegal growers cultivate indoors using artificial lights. This helps avoid detection but reduces the CBD production of the plant.
Australia's National Cannabis Prevention and Information Centre (NCPIC) states that the buds (flowers) of the female cannabis plant contain the highest concentration of THC, followed by the leaves. The stalks and seeds have "much lower THC levels". The UN states that leaves can contain ten times less THC than the buds, and the stalks one hundred times less THC.
After revisions to cannabis rescheduling in the UK, the government moved cannabis back from a class C to a class B drug. A purported reason was the appearance of high potency cannabis. They believe skunk accounts for between 70 and 80% of samples seized by police (despite the fact that skunk can sometimes be incorrectly mistaken for all types of herbal cannabis). Extracts such as hashish and hash oil typically contain more THC than high potency cannabis flowers.
Marijuana
Marijuana or marihuana (herbal cannabis), consists of the dried flowers and subtending leaves and stems of the female Cannabis plant. This is the most widely consumed form, containing 3% to 20% THC, with reports of up-to 33% THC. This is the stock material from which all other preparations are derived. Although herbal cannabis and industrial hemp derive from the same species and contain the psychoactive component (THC), they are distinct strains with unique biochemical compositions and uses. Hemp has lower concentrations of THC and higher concentrations of cannabidiol (CBD), which decreases the psychoactive effects
Kief
Kief is a powder, rich in trichomes, which can be sifted from the leaves and flowers of cannabis plants and either consumed in powder form or compressed to produce cakes of hashish. The word "kif" derives from colloquial Arabic كيف kēf/kīf, meaning pleasure.
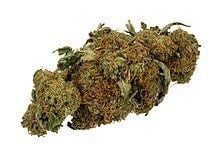
Hashish
Hashish (also spelled hasheesh, hashisha, or simply hash) is a concentrated resin cake or ball produced from pressed kief, the detached trichomes and fine material that falls off cannabis flowers and leaves. or from scraping the resin from the surface of the plants and rolling it into balls. It varies in color from black to golden brown depending upon purity and variety of cultivar it was obtained from. It can be consumed orally or smoked, and is also vaporised, or 'vaped'. The term "Rosin Hash" refers to a high quality solventless product obtained through heat and pressure.
Tincture
Cannabinoids can be extracted from cannabis plant matter using high-proof spirits (often grain alcohol) to create a tincture, often referred to as "green dragon". Nabiximols is a branded product name from a tincture manufacturing pharmaceutical company.
Hash oil
Hash oil is a resinous matrix of cannabinoids obtained from the Cannabis plant by solvent extraction, formed into a hardened or viscous mass. Hash oil can be the most potent of the main cannabis products because of its high level of psychoactive compound per its volume, which can vary depending on the plant's mix of essential oils and psychoactive compounds. Butane and supercritical carbon dioxide hash oil have become popular in recent years. Some drug dealers add other illegal drugs to products sold as hash oil.
Infusions
There are many varieties of cannabis infusions owing to the variety of non-volatile solvents used. The plant material is mixed with the solvent and then pressed and filtered to express the oils of the plant into the solvent. Examples of solvents used in this process are cocoa butter, dairy butter, cooking oil, glycerine, and skin moisturizers. Depending on the solvent, these may be used in cannabis foods or applied topically.
Adulterated cannabis
Contaminants or adulterants may be found in marijuana or hashish. Other substances may be added to cannabis to add weight to the product (lead has been used in some cases), to increase its psychoactive effects (e.g., Phencyclidine), or as part of the cultivation and processing of the cannabis (e.g., fertilizer). Hashish obtained from "soap bar"-type sources. The dried flowers of the plant may be contaminated by the plant taking up heavy metals and other toxins from its growing environment, or by the addition of glass. In the Netherlands, chalk has been used to make cannabis appear to be of a higher quality. Increasing the weight of hashish products in Germany with lead caused lead intoxication in at least 29 users.
Despite cannabis being generally perceived as a natural product, in a recent Australian survey one in four Australians consider cannabis grown indoors under hydroponic conditions to be a greater health risk due to increased contamination, added to the plant during cultivation to enhance the plant growth and quality.
Drug dealers may "spike" or lace marijuana with other chemicals such as PCP, creating a product known as "wet marijuana"; this enhances the effects of smoking it and it can be used to make low-grade, low-potency marijuana seem more effective.
Medical use
Medical marijuana refers to the use of the Cannabis plant as a physician-recommended herbal therapy as well as synthetic THC and cannabinoids. So far, the medical use of cannabis is legal only in a limited number of territories, including Canada, Belgium, Australia, the Netherlands, Spain, and several U.S. states. This usage generally requires a prescription, and distribution is usually done within a framework defined by local laws. There is evidence supporting the use of cannabis or its derivatives in the treatment of chemotherapy-induced nausea and vomiting, neuropathic pain, and multiple sclerosis. Lower levels of evidence support its use for AIDS wasting syndrome, epilepsy, rheumatoid arthritis, and glaucoma.
History
Cannabis is indigenous to Central and South Asia. There is evidence of inhalation of cannabis smoke from the 3rd millennium BCE, namely charred cannabis seeds found in a ritual brazier at an ancient burial site in present-day Romania. The earliest written reference to cannabis dates back to 2727 B.C., from the Chinese emperor Shennong.
In 2003, a leather basket filled with cannabis leaf fragments and seeds was found next to a 2,500- to 2,800-year-old mummified shaman in the northwestern Xinjiang Uygur Autonomous Region of China. Evidence of cannabis consumption was also found in Egyptian mummies dated about 950 BC.
Hemp is called ganja (Sanskrit: गञ्जा, IAST: gañjā) in Sanskrit and other modern Indo-Aryan languages. Some scholars suggest that the ancient drug soma, mentioned in the Vedas, was cannabis, although this theory is disputed.
Cannabis was also known to the ancient Assyrians, who discovered its psychoactive properties through the Aryans. Using it in some religious ceremonies, they called it qunubu (meaning "way to produce smoke"), a probable origin of the modern word "cannabis". The Aryans also introduced cannabis to the Scythians, Thracians and Dacians, whose shamans (the kapnobatai—"those who walk on smoke/clouds") burned cannabis flowers to induce trance.
Cannabis has an ancient history of ritual use and is found in pharmacological cults around the world. Hemp seeds discovered by archaeologists at Pazyryk suggest early ceremonial practices like eating by the Scythians occurred during the 5th to 2nd century BCE, confirming previous historical reports by Herodotus. It was used by Muslims in various Sufi orders as early as the Mamluk period, for example by the Qalandars. Smoking pipes uncovered in Ethiopia and carbon-dated to around 1320 CE were found to have traces of cannabis.
A study published in the South African Journal of Science showed that "pipes dug up from the garden of Shakespeare's home in Stratford-upon-Avon contain traces of cannabis." The chemical analysis was carried out after researchers hypothesized that the "noted weed" mentioned in Sonnet 76 and the "journey in my head" from Sonnet 27 could be references to cannabis and the use thereof. Examples of classic literature featuring cannabis include Les paradis artificiels by Charles Baudelaire and The Hasheesh Eater by Fitz Hugh Ludlow.
In the mid-1800s, Irish physician William Brooke O'Shaughnessy, who had studied the drug while working as a medical officer in Bengal with the East India company, brought a quantity of cannabis with him on his return to Britain in 1842, provoking renewed interest in the West.
John Gregory Bourke described the use of "mariguan", which he identifies as Cannabis indica or Indian hemp, by Mexican residents of the Rio Grande region of Texas in 1894. He described its uses for treatment of asthma, to expedite delivery, to keep away witches, and as a love-philtre. He also wrote that many Mexicans added the herb to their cigarritos or mescal, often taking a bite of sugar afterward to intensify the effect. Bourke wrote that because it was often used in a mixture with toloachi (which he inaccurately describes as Datura stramonium), mariguan was one of the several plants known as "loco weed". Bourke compared mariguan to hasheesh, which he called "one of the greatest curses of the East", citing reports that users "become maniacs and are apt to commit all sorts of acts of violence and murder", causing degeneration of the body and an idiotic appearance, and mentioned laws against sale of hasheesh "in most Eastern countries".
Cannabis was criminalized in various countries beginning in the early 20th century. In the United States, the first restrictions on sale of cannabis came in 1906 (in District of Columbia). It was outlawed Jamaica (then a British colony) in 1913, in South Africa in 1922, and in the United Kingdom and New Zealand in the 1920s. Canada criminalized cannabis in the Opium and Drug Act of 1923, before any reports of the use of the drug in Canada. In 1925 a compromise was made at an international conference in The Hague about the International Opium Convention that banned exportation of "Indian hemp" to countries that had prohibited its use, and requiring importing countries to issue certificates approving the importation and stating that the shipment was required "exclusively for medical or scientific purposes". It also required parties to "exercise an effective control of such a nature as to prevent the illicit international traffic in Indian hemp and especially in the resin".
In the United States in 1937, the Marihuana Tax Act was passed, and prohibited the production of hemp in addition to cannabis. The reasons that hemp was also included in this law are disputed—several scholars have claimed that the act was passed in order to destroy the US hemp industry, with the primary involvement of businessmen Andrew Mellon, Randolph Hearst, and the Du Pont family. But the improvements of the decorticators, machines that separate the fibers from the hemp stem, could not make hemp fiber a very cheap substitute for fibers from other sources because it could not change that basic fact that strong fibers are only found in the bast, the outer part of the stem. Only about 1/3 of the stem are long and strong fibers. The company DuPont and many industrial historians dispute a link between nylon and hemp. They argue that the purpose of developing the nylon was to produce a fiber that could be used in thin stockings for females and compete with silk.
The United Nations' 2012 Global Drug Report stated that cannabis "was the world's most widely produced, trafficked, and consumed drug in the world in 2010", identifying that between 119 million and 224 million users existed in the world's adult (18 or older) population.
Legal status
Since the beginning of the 20th century, most countries have enacted laws against the cultivation, possession or transfer of cannabis. These laws have impacted adversely on the cannabis plant's cultivation for non-recreational purposes, but there are many regions where, under certain circumstances, handling of cannabis is legal or licensed. Many jurisdictions have lessened the penalties for possession of small quantities of cannabis so that it is punished by confiscation and sometimes a fine, rather than imprisonment, focusing more on those who traffic the drug on the black market.
In some areas where cannabis use has been historically tolerated, some new restrictions have been put in place, such as the closing of cannabis coffee shops near the borders of the Netherlands, closing of coffee shops near secondary schools in the Netherlands and crackdowns on "Pusher Street" in Christiania, Copenhagen in 2004.
Some jurisdictions use free voluntary treatment programs and/or mandatory treatment programs for frequent known users. Simple possession can carry long prison terms in some countries, particularly in East Asia, where the sale of cannabis may lead to a sentence of life in prison or even execution. More recently, however, many political parties, non-profit organizations, and causes based on the legalization of medical cannabis and/or legalizing the plant entirely (with some restrictions) have emerged.
In December 2012, the U.S. state of Washington became the first state to officially legalize cannabis in a state law (Washington Initiative 502) (but still illegal by federal law), with the state of Colorado following close behind (Colorado Amendment 64). On January 1, 2013, the first marijuana "club" for private marijuana smoking (no buying or selling, however) was allowed for the first time in Colorado. The California Supreme Court decided in May 2013 that local governments can ban medical marijuana dispensaries despite a state law in California that permits the use of cannabis for medical purposes. At least 180 cities across California have enacted bans in recent years.
In December 2013, Uruguay became the first country to legalize growing, sale and use of cannabis. However, as of August 2014, no cannabis has yet been sold legally in Uruguay. According to the law, the only cannabis that can be sold legally must be grown in the country by no more than five licensed growers, and these have yet to be selected; in fact, the call for applications did not go out until August 1, 2014.
On October 17, 2015, Australian health minister Sussan Ley presented a new law that will allow the cultivation of cannabis for scientific research and medical trials on patients. In December 2015, it was reported that the Canadian government had committed to legalizing cannabis, but at that time no timeline for the legalization was set out.
As drugs has increasingly come to be seen as a health issue instead of criminal behavior, marijuana has also been legalized or decriminalized in: Czech Republic, Colombia, Ecuador, Mexico, Portugal, and Canada.
Usage
In 2013, between 128 and 232 million people used cannabis (2.7% to 4.9% of the global population between the ages of 15 and 65). Cannabis is by far the most widely used illicit substance.
United States
Between 1973 and 1978, eleven states decriminalized marijuana. In 2001 Nevada reduced marijuana possession to a misdemeanor and since 2012, several other states have decriminalized and even legalized marijuana.
In 2015, almost half of the people in the United States had tried marijuana, 12% had used it in the past year, and 7.3% had used it in the past month. In 2014, daily marijuana use amongst US college students had reached its highest level since records began in 1980, rising from 3.5% in 2007 to 5.9% in 2014 and had surpassed daily cigarette use.
In the US, men are over twice as likely to use marijuana as women and 18-29 year-olds are six times more likely to use as over 65-year-olds. In 2015, a record 44% of the US population has tried marijuana in their lifetime, an increase from 38% in 2013 and 33% in 1985.
Marijuana use in the United States is three times above the global average, but in line with other Western democracies. 44% of American 12th graders have tried the drug at least once, and the typical age of first-use is 16, similar to the typical age of first-use for alcohol but lower than the first-use age for other illicit drugs.
Production
It is often claimed by growers and breeders of herbal cannabis that advances in breeding and cultivation techniques have increased the potency of cannabis since the late 1960s and early '70s when THC was first discovered and understood. However, potent seedless cannabis such as "Thai sticks" were already available at that time. Sinsemilla (Spanish for "without seed") is the dried, seedless inflorescences of female cannabis plants. Because THC production drops off once pollination occurs, the male plants (which produce little THC themselves) are eliminated before they shed pollen to prevent pollination. Advanced cultivation techniques such as hydroponics, cloning, high-intensity artificial lighting, and the sea of green method are frequently employed as a response (in part) to prohibition enforcement efforts that make outdoor cultivation more risky. It is often cited that the average levels of THC in cannabis sold in the United States rose dramatically between the 1970s and 2000, but such statements are likely skewed because undue weight is given to much more expensive and potent, but less prevalent samples.
"Skunk" refers to several named strains of potent cannabis, grown through selective breeding and sometimes hydroponics. It is a cross-breed of Cannabis sativa and C. indica (although other strains of this mix exist in abundance). Skunk cannabis potency ranges usually from 6% to 15% and rarely as high as 20%. The average THC level in coffee shops in the Netherlands is about 18–19%.
Price
The price or street value of cannabis varies widely depending on geographic area and potency.
In the United States, cannabis is overall the number four value crop, and is number one or two in many states including California, New York and Florida, averaging $3,000/lb. Some believe it generates an estimated $36 billion market. Some have argued that this estimate is methodologically flawed, and makes unrealistic assumptions about the level of marijuana consumption. Other estimates claiming to correct for this flaw claim that the market is between $2.1-$4.3 billion. The United Nations Office on Drugs and Crime claims in its 2008 World Drug Report that typical U.S. retail prices are $10–15 per gram (approximately $280–420 per ounce). Street prices in North America are known to range from about $40 to $400 per ounce, depending on quality.
The European Monitoring Centre for Drugs and Drug Addiction reports that typical retail prices in Europe for cannabis varies from €2 to €20 per gram, with a majority of European countries reporting prices in the range €4–10.
Distribution
Marijuana vending machines for selling or dispensing cannabis are in use in the United States and are planned to be used in Canada.
Gateway drug
The Gateway Hypothesis states that cannabis use increases the probability of trying "harder" drugs. The hypothesis has been hotly debated as it is regarded by some as the primary rationale for the United States prohibition on cannabis use. A Pew Research Center poll found that political opposition to marijuana use was significantly associated with concerns about health effects and whether legalization would increase marijuana use by children.
Some studies state that while there is no proof for the gateway hypothesis, young cannabis users should still be considered as a risk group for intervention programs. Other findings indicate that hard drug users are likely to be poly-drug users, and that interventions must address the use of multiple drugs instead of a single hard drug. Almost two-thirds of the poly drug users in the "2009/10 Scottish Crime and Justice Survey" used cannabis.
The gateway effect may appear due to social factors involved in using any illegal drug. Because of the illegal status of cannabis, its consumers are likely to find themselves in situations allowing them to acquaint with individuals using or selling other illegal drugs. Utilizing this argument some studies have shown that alcohol and tobacco may additionally be regarded as gateway drugs; however, a more parsimonious explanation could be that cannabis is simply more readily available (and at an earlier age) than illegal hard drugs. In turn alcohol and tobacco are easier to obtain at an earlier point than is cannabis (though the reverse may be true in some areas), thus leading to the "gateway sequence" in those individuals since they are most likely to experiment with any drug offered.
An alternative to the gateway hypothesis is the common liability to addiction (CLA) theory. It states that some individuals are, for various reasons, willing to try multiple recreational substances. The "gateway" drugs are merely those that are (usually) available at an earlier age than the harder drugs. Researchers have noted in an extensive review, Vanyukov et al., that it is dangerous to present the sequence of events described in gateway "theory" in causative terms as this hinders both research and intervention.
Research
Cannabis research is challenging since the plant is illegal in most countries. Research-grade samples of the drug are difficult to obtain for research purposes, unless granted under authority of national governments.
There are also other difficulties in researching the effects of cannabis. Many people who smoke cannabis also smoke tobacco. This causes confounding factors, where questions arise as to whether the tobacco, the cannabis, or both that have caused a cancer. Another difficulty researchers have is in recruiting people who smoke cannabis into studies. Because cannabis is an illegal drug in many countries, people may be reluctant to take part in research, and if they do agree to take part, they may not say how much cannabis they actually smoke.
A 2015 review found that the use of high cannabidiol-to-THC strains of cannabis showed significantly fewer positive symptoms such as delusions and hallucinations, better cognitive function and both lower risk for developing psychosis, as well as a later age of onset of the illness, compared to cannabis with low CBD-to-THC ratios. A 2014 Cochrane review found that research was insufficient to determine the safety and efficacy to using cannabis to treat schizophrenia or psychosis.