
MeSH D015190 | ||
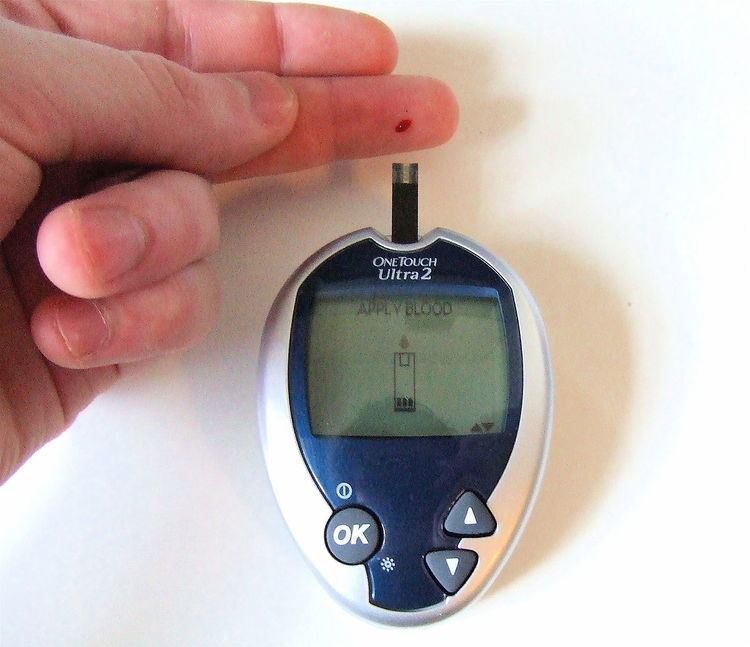 | ||
Blood glucose monitoring is a way of testing the concentration of glucose in the blood (glycemia). Particularly important in the care of diabetes mellitus, a blood glucose test is performed by piercing the skin (typically, on the finger) to draw blood, then applying the blood to a chemically active disposable 'test-strip'. Different manufacturers use different technology, but most systems measure an electrical characteristic, and use this to determine the glucose level in the blood. The test is usually referred to as capillary blood glucose.
Contents
- Purpose
- Blood glucose meters
- Continuous glucose monitoring
- Glucose sensing bio implants
- Non invasive technologies
- Effectiveness
- Blood glucose monitoring recommendations
- References
Healthcare professionals advise patients with diabetes on the appropriate monitoring regimen for their condition. Most people with Type 2 diabetes test at least once per day. Diabetics who use insulin (all Type 1 diabetes and many Type 2s) usually test their blood sugar more often (3 to 10 times per day), both to assess the effectiveness of their prior insulin dose and to help determine their next insulin dose.
Improved technology for measuring blood glucose is rapidly changing the standards of care for all diabetic people.
Purpose
Blood glucose monitoring reveals individual patterns of blood glucose changes, and helps in the planning of meals, activities, and at what time of day to take medications.
Also, testing allows for quick response to high blood sugar (hyperglycemia) or low blood sugar (hypoglycemia). This might include diet adjustments, exercise, and insulin (as instructed by the health care provider).
Blood glucose meters
A blood glucose meter is an electronic device for measuring the blood glucose level. A relatively small drop of blood is placed on a disposable test strip which interfaces with a digital meter. Within several seconds, the level of blood glucose will be shown on the digital display.
Needing only a small drop of blood for the meter means that the time and effort required for testing is reduced and the compliance of diabetic people to their testing regimens is improved. Although the cost of using blood glucose meters seems high, it is believed to be a cost benefit relative to the avoided medical costs of the complications of diabetes.
Recent advances include:
Continuous glucose monitoring
A continuous glucose monitor (CGM) determines glucose levels on a continuous basis (every few minutes). A typical system consists of:
Continuous glucose monitors measure the glucose level of interstitial fluid. Shortcomings of CGM systems due to this fact are:
Patients therefore require traditional fingerstick measurements for calibration (typically twice per day) and are often advised to use fingerstick measurements to confirm hypo- or hyperglycemia before taking corrective action.
The lag time discussed above has been reported to be about 5 minutes. Anecdotally, some users of the various systems report lag times of up to 10–15 minutes. This lag time is insignificant when blood sugar levels are relatively consistent. However, blood sugar levels, when changing rapidly, may read in the normal range on a CGM system while in reality the patient is already experiencing symptoms of an out-of-range blood glucose value and may require treatment. Patients using CGM are therefore advised to consider both the absolute value of the blood glucose level given by the system as well as any trend in the blood glucose levels. For example, a patient using CGM with a blood glucose of 100 mg/dl on their CGM system might take no action if their blood glucose has been consistent for several readings, while a patient with the same blood glucose level but whose blood glucose has been dropping steeply in a short period of time might be advised to perform a fingerstick test to check for hypoglycemia.
Continuous monitoring allows examination of how the blood glucose level reacts to insulin, exercise, food, and other factors. The additional data can be useful for setting correct insulin dosing ratios for food intake and correction of hyperglycemia. Monitoring during periods when blood glucose levels are not typically checked (e.g. overnight) can help to identify problems in insulin dosing (such as basal levels for insulin pump users or long-acting insulin levels for patients taking injections). Monitors may also be equipped with alarms to alert patients of hyperglycemia or hypoglycemia so that a patient can take corrective action(s) (after fingerstick testing, if necessary) even in cases where they do not feel symptoms of either condition. While the technology has its limitations, studies have demonstrated that patients with continuous sensors experience less hyperglycemia and also reduce their glycosylated hemoglobin levels.
Currently, continuous blood glucose monitoring is not automatically covered by health insurance in the United States in the same way that most other diabetic supplies are covered (e.g. standard glucose testing supplies, insulin, and even insulin pumps). However, an increasing number of insurance companies do cover continuous glucose monitoring supplies (both the receiver and disposable sensors) on a case-by-case basis if the patient and doctor show a specific need. The lack of insurance coverage is exacerbated by the fact that disposable sensors must be frequently replaced. Some sensors have been U.S. Food and Drug Administration (FDA) approved for 7- and 3-day use, though some patients wear sensors for longer than the recommended period) and the receiving meters likewise have finite lifetimes (less than 2 years and as little as 6 months). This is one factor in the slow uptake in the use of sensors that have been marketed in the United States.
The principles, history and recent developments of operation of electrochemical glucose biosensors are discussed in a chemical review by Joseph Wang.
Some projects such Nightscout (DIY) allow parents to have a permanent control of glucose levels on their children from devices such cellphones, tablets, laptops, pebble watch, etc.
Glucose sensing bio-implants
Investigations on the use of test strips have shown that the required self-injury acts as a psychological barrier restraining the patients from sufficient glucose control. As a result, secondary diseases are caused by excessive glucose levels. A significant improvement of diabetes therapy might be achieved with an implantable sensor that would continuously monitor blood sugar levels within the body and transmit the measured data outside. The burden of regular blood testing would be taken from the patient, who would instead follow the course of their glucose levels on an intelligent device like a laptop or a smart phone.
Glucose concentrations do not necessarily have to be measured in blood vessels, but may also be determined in the interstitial fluid, where the same levels prevail – with a time lag of a few minutes – due to its connection with the capillary system. However, the enzymatic glucose detection scheme used in single-use test strips is not directly suitable for implants. One main problem is caused by the varying supply of oxygen, by which glucose is converted to glucono lactone and H2O2 by glucose oxidase. Since the implantation of a sensor into the body is accompanied by growth of encapsulation tissue, the diffusion of oxygen to the reaction zone is continuously diminished. This decreasing oxygen availability causes the sensor reading to drift, requiring frequent re-calibration using finger-sticks and test strips.
One approach to achieving long-term glucose sensing is to measure and compensate for the changing local oxygen concentration. Other approaches replace the troublesome glucose oxidase reaction with a reversible sensing reaction, known as an affinity assay. This scheme was originally put forward by Schultz & Sims in 1978. A number of different affinity assays have been investigated, with fluorescent assays proving most common. MEMS technology has recently allowed for smaller and more convenient alternatives to fluorescent detection, via measurement of viscosity. Investigation of affinity-based sensors has shown that encapsulation by body tissue does not cause a drift of the sensor signal, but only a time lag of the signal compared to the direct measurement in blood.
Non-invasive technologies
Some new technologies to monitor blood glucose levels will not require access to blood to read the glucose level. Non-invasive technologies include near IR detection, ultrasound and dielectric spectroscopy. These may free the person with diabetes from finger sticks to supply the drop of blood for blood glucose analysis.
Most of the non-invasive methods under development are continuous glucose monitoring methods and offer the advantage of providing additional information to the subject between the conventional finger stick, blood glucose measurements and over time periods where no finger stick measurements are available (i.e. while the subject is sleeping).
Effectiveness
For patients with diabetes mellitus type 2, the importance of monitoring and the optimal frequency of monitoring are not clear. A 2011 study found no evidence that blood glucose monitoring leads to better patient outcomes in actual practice. One randomized controlled trial found that self-monitoring of blood glucose did not improve glycosylated hemoglobin (HbA1c) among "reasonably well controlled non-insulin treated patients with type 2 diabetes". However a recent meta-analysis of 47 randomized controlled trials encompassing 7677 patients showed that self-care management intervention improves glycemic control in diabetics, with an estimated 0.36% (95% CI, 0.21-0.51) reduction in their glycosylated hemoglobin values. Furthermore, a recent study showed that patients described as being "Uncontrolled Diabetics" (defined in this study by HbA1C levels >8%) showed a statistically significant decrease in the HbA1C levels after a 90-day period of seven-point self-monitoring of blood glucose (SMBG) with a relative risk reduction (RRR) of 0.18% (95% CI, 0.86-2.64%, p<.001). Regardless of lab values or other numerical parameters, the purpose of the clinician is to improve quality of life and patient outcomes in diabetic patients. A recent study included 12 randomized controlled trials and evaluated outcomes in 3259 patients. The authors concluded through a qualitative analysis that SMBG on quality of life showed no effect on patient satisfaction or the patients' health-related quality of life. Furthermore, the same study identified that patients with type 2 diabetes mellitus diagnosed greater than one year prior to initiation of SMBG, who were not on insulin, experienced a statistically significant reduction in their HbA1C of 0.3% (95% CI, -0.4 - -0.1) at six months follow up, but a statistically insignificant reduction of 0.1% (95% CI, -0.3 – 0.04) at twelve months follow up. Conversely, newly diagnosed patients experienced a statistically significant reduction of 0.5% (95% CI, -0.9 – -0.1) at 12 months follow up. A recent study found that a treatment strategy of intensively lowering blood sugar levels (below 6%) in patients with additional cardiovascular disease risk factors poses more harm than benefit. For type 2 diabetics who are not on insulin, exercise and diet are the best tools. Blood glucose monitoring is, in that case, simply a tool to evaluate the success of diet and exercise. Insulin-dependent type 2 diabetics do not need to monitor their blood sugar as frequently as type 1 diabetics.
Blood glucose monitoring recommendations
The National Institute for Health and Clinical Excellence (NICE), UK released updated diabetes recommendations on 30 May 2008, which recommend that self-monitoring of plasma glucose levels for people with newly diagnosed type 2 diabetes must be integrated into a structured self-management education process. The recommendations have been updated in August 2015 for children and young adults with type 1 diabetes. See: NICE Guideline for Continuous Blood Glucose Monitoring.