
Specialty medical genetics ICD-9-CM 753.1 DiseasesDB 10280 | ICD-10 Q61 OMIM 263200 MedlinePlus 000502 | |
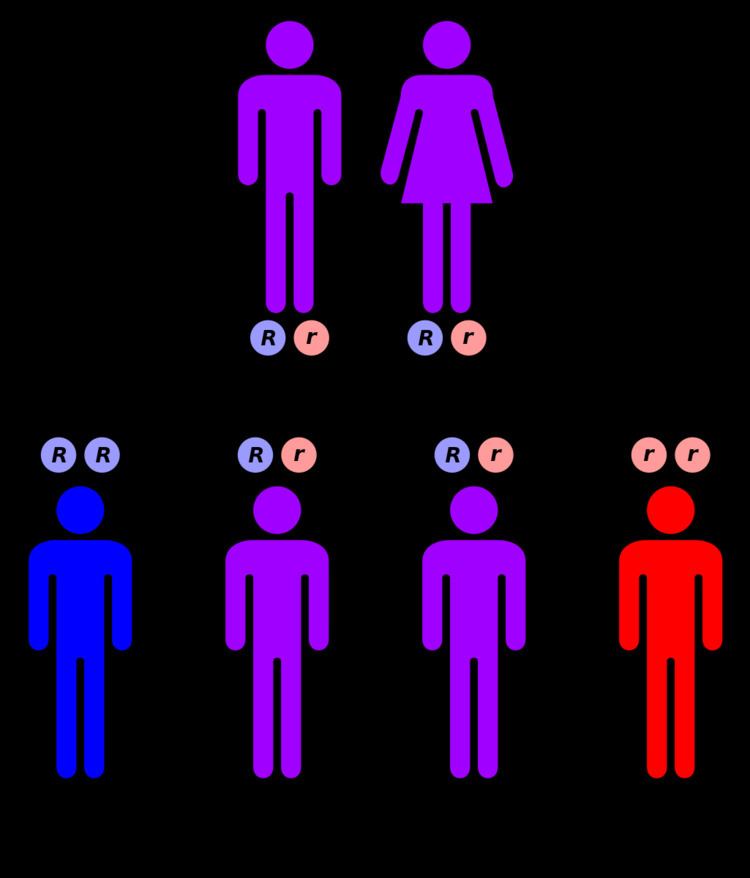 | ||
Autosomal recessive polycystic kidney disease (ARPKD) is the recessive form of polycystic kidney disease. It is associated with a group of congenital fibrocystic syndromes. Mutations in the PKHD1 (chromosomal locus 6p12.2) cause ARPKD.
Contents
Signs and symptoms
Symptoms and signs include abdominal discomfort, polyuria, polydipsia, incidental discovery of hypertension, abdominal mass. The classic presentation for ARPKD is systemic hypertension with progression to end-stage renal disease (ESRD) by the age of 15. In atypical presentation, a small number of ARPKD sufferers live to adulthood with some kidney function; but with significant deterioration in liver function. This outcome is postulated to result from expression of the polycystic kidney and hepatic disease gene PKHD1, which is located on chromosome 6p. In severe cases, a fetus will present with oligohydramnios and as a result, may present with Potter sequence.
Genetics
The cause of ARPKD is linked to mutations in the PKHD1 gene.
ARPKD is a significant hereditary renal disease in that appears in childhood. The prevalence is estimated to be of 1 in 20,000 live births. With a reported carrier frequency of up to 1:70. The single gene mutation called ‘’PKHD1’’ is fully responsible for the disease presentation of ARPKD. This PKHD1 is located on the human chromosome region 6p21.1-6p12.2. It is also one of the largest genes in the genome as it occupies approximately 450 kb of DNA, and contains at least 86 exons.
It is capable of producing multiple alternatively spliced transcripts. The largest known transcript encodes fibrocystin /polyductin (FPC), which is a large receptor-like integral membrane protein of 4074 amino acids. The structure of the FPC consist of a single transmembrane, a large N-terminal extracellular region, and a short intracellular cytoplasmic domain. The FPC protein is found on the primary cilia of epithelia cells of cortical and medullary collecting ducts and cholangiocytes of bile ducts, and show similarity to polycystins and several other ciliopathy proteins. FPC is also found to be expressed on the basal body and plasma membrane. It is presumed that the large extracellular domain of FPC binds to a ligand(s) that is yet unknown and that is also involved in cell-cell and cell-matrix interactions.
It is known that FPC interacts with ADPKD protein PC2 and may also participate in this regulation pathway of the mechanosensory function of the primary cilia, calcium signaling, and PCP. This is suggesting a common mechanism underlying cystogenesis between ADPKD and ARPKD. The FPC protein is also found on the centrosomes and mitotic spindle and may regulate centrosome duplication and mitotic spindle assembly during cell division. There have been a large number of various single gene mutations found throughout PKHD1 and are unique to individual families. Most of the patients are compound heterozygotes for PKHD1 mutations. Patients with two nonsense mutations appear to have an earlier onset of the disease.
Diagnosis
Ultrasonography is the primary method to evaluate ARPKD, particularly in the perinatal and neonatal.
Treatment
The treatment options for autosomal recessive polycystic kidney disease, given there is no current cure, are: