
Specialty cardiology DiseasesDB 33437 MeSH D020759 | ICD-10 I65.8 eMedicine neuro/348 | |
 | ||
ICD-9-CM 433.8 806.02, 806.07, 806.12, 806.17, 806.22, 806.27, 806.32, 806.37 | ||
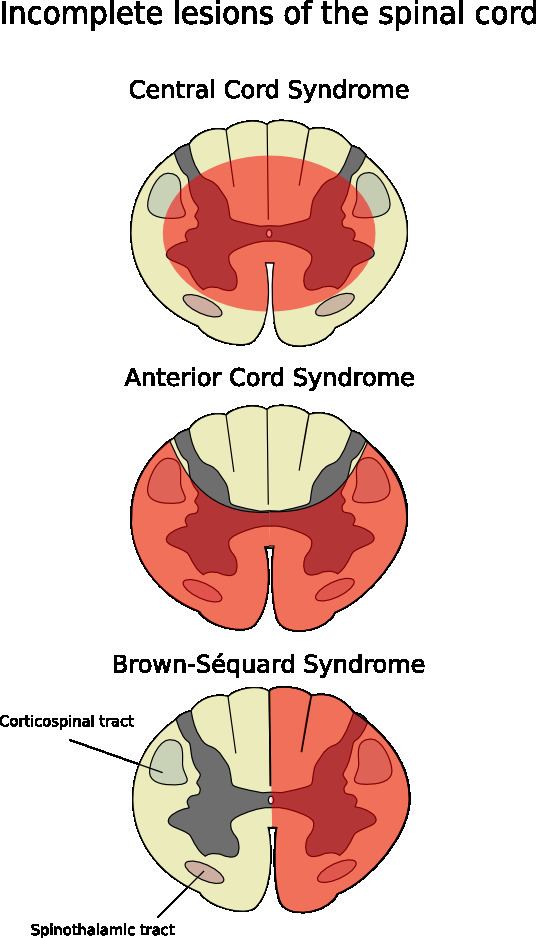
Anterior spinal artery syndrome (also known as "anterior spinal cord syndrome") is a medical condition where the anterior spinal artery, the primary blood supply to the anterior portion of the spinal cord, is interrupted, causing ischemia or infarction of the spinal cord in the anterior two-thirds of the spinal cord and medulla oblongata. It is characterized by loss of motor function below the level of injury, loss of sensations carried by the anterior columns of the spinal cord (pain and temperature), and preservation of sensations carried by the posterior columns (fine touch, vibration and proprioception). Anterior spinal artery syndrome is the most common form of spinal cord infarction.
Contents
Anatomy
The anterior portion of the spinal cord is supplied by the anterior spinal artery. It begins at the foramen magnum where branches of the two vertebral arteries exit, merge, and descend along the anterior spinal cord. As the anterior spinal artery proceeds inferiorly, it receives branches originating mostly from the aorta. The largest aortic branch is the artery of Adamkiewicz.
Signs and symptoms
Symptoms usually occur very quickly and are often experienced within one hour of the initial damage. MRI can detect the magnitude and location of the damage 10–15 hours after the initiation of symptoms. Diffusion-weighted imaging may be used as it is able to identify the damage within a few minutes of symptomatic onset.
Clinical features include paraparesis or quadriparesis (depending on the level of the injury) and impaired pain and temperature sensation. Complete motor paralysis below the level of the lesion due to interruption of the corticospinal tract, and loss of pain and temperature sensation at and below the level of the lesion. Proprioception and vibratory sensation is preserved, as it is in the dorsal side of the spinal cord.
Causes
Due to the branches of the aorta that supply the anterior spinal artery, the most common causes are insufficiencies within the aorta. These include aortic aneurysms, dissections, direct trauma to the aorta, surgeries, and atherosclerosis. Acute disc herniation, cervical spondylosis, kyphoscoliosis, damage to the spinal column and neoplasia all could result in ischemia from anterior spinal artery occlusion leading to anterior cord syndrome. Other causes include vasculitis, polycythemia, sickle cell disease, decompression sickness, and collagen and elastin disorders.
Treatment and prognosis
Treatment is determined based on the primary cause of anterior cord syndrome. When the diagnosis of anterior cord syndrome is determined, the prognosis is unfortunate. The mortality rate is approximately 20%, with 50% of individuals living with anterior cord syndrome having very little or no changes in symptoms.
Eponym
It is also known as "Beck's syndrome".