
NeuroNames ancil-114 FMA 72644 | TA A14.1.04.138 | |
 | ||
Latin Tractus spinothalamicus | ||
The spinothalamic tract (also known as anterolateral system or the ventrolateral system) is a sensory pathway from the skin to the thalamus. From the ventral posterolateral nucleus in the thalamus, sensory information is relayed upward to the somatosensory cortex of the postcentral gyrus.
Contents
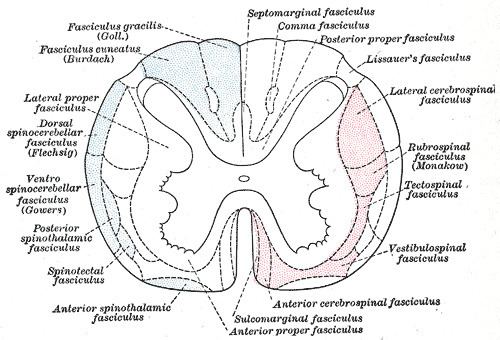
The spinothalamic tract consists of two adjacent pathways: anterior and lateral. The anterior spinothalamic tract carries information about crude touch. The lateral spinothalamic tract conveys pain and temperature.
In the spinal cord, the spinothalamic tract has somatotopic organization. This is the segmental organization of its cervical, thoracic, lumbar, and sacral components, which is arranged from most medial to most lateral respectively.
The pathway decussates at the level of the spinal cord, rather than in the brainstem like the posterior column-medial lemniscus pathway and lateral corticospinal tract.
Structure
There are two main parts of the spinothalamic tract (STT):
The spinothalamic tract, like the dorsal column-medial lemniscus tract, uses three neurons to convey sensory information from the periphery to conscious level at the cerebral cortex.
Pseudounipolar neurons in the dorsal root ganglion have axons that lead from the skin into the dorsal spinal cord where they ascend or descend one or two vertebral levels via Lissauer's tract and then synapse with secondary neurons in either the substantia gelatinosa of Rolando or the nucleus proprius. These secondary neurons are called tract cells.
The axons of the tract cells cross over (decussate) to the other side of the spinal cord via the anterior white commissure, and to the anterolateral corner of the spinal cord (hence the spinothalamic tract being part of the anterolateral system). Decussation usually occurs 1-2 spinal nerve segments above the point of entry. The axons travel up the length of the spinal cord into the brainstem, specifically the rostral ventromedial medulla.
Traveling up the brainstem, the tract moves dorsally. The neurons ultimately synapse with third-order neurons in several nuclei of the thalamus—including the medial dorsal, ventral posterior lateral, and ventral posterior medial nuclei. From there, signals go to the cingulate cortex, the primary somatosensory cortex, and insular cortex respectively.
Function
The types of sensory information transmitted via the spinothalamic tract are described as affective sensation. This means that the sensation is accompanied by a compulsion to act. For instance, an itch is accompanied by a need to scratch, and a painful stimulus makes us want to withdraw from the pain.
There are two sub-systems identified:
Anterolateral system
In the nervous system, the anterolateral system is an ascending pathway that conveys pain, temperature (protopathic sensation), and crude touch from the periphery to the brain. It comprises three main pathways:
Clinical significance
In contrast to the axons of second-order neurons in posterior column-medial lemniscus pathway, the axons of second-order neurons in the spinothalamic tracts cross at every segmental level in the spinal cord. This fact aids in determining whether a lesion is in the brain or the spinal cord. With lesions in the brain stem or higher, deficits of pain perception, touch sensation, and proprioception are all contralateral to the lesion. With spinal cord lesions, however, the deficit in pain perception is contralateral to the lesion, whereas the other deficits are ipsilateral. See Brown-Séquard syndrome.
Unilateral lesions usually cause contralateral anaesthesia (loss of pain and temperature). Anaesthesia will normally begin 1-2 segments below the level of lesion, affecting all caudal body areas. This is clinically tested by using pin pricks.