
Specialty gastroenterology | ICD-10 K59.8 | |
 | ||
Anismus (or dyssynergic defecation) refers to the failure of the normal relaxation of pelvic floor muscles during attempted defecation.
Contents
- Etymology and synonyms
- Definition
- Classification
- Signs and symptoms
- Cause
- Complications
- Diagnosis
- Digital rectal examination
- Anorectal manometry
- Evacuation proctography
- Balloon expulsion test
- Rectal cooling test
- Treatment
- References
Anismus can occur in both children and adults, and in both men and women (although it is more common in women). It can be caused by physical defects or it can occur for other reasons or unknown reasons. Anismus that has a behavioral cause could be viewed as having similarities with parcopresis, or psychogenic fecal retention.
Symptoms include tenesmus (the sensation of incomplete emptying of the rectum after defecation has occurred) and constipation. Retention of stool may result in fecal loading (retention of a mass of stool of any consistency) or fecal impaction (retention of a mass of hard stool). This mass may stretch the walls of the rectum and colon, causing megarectum and/or megacolon, respectively. Liquid stool may leak around a fecal impaction, possibly causing degrees of liquid fecal incontinence. This is usually termed encopresis or soiling in children, and fecal leakage, soiling or liquid fecal incontinence in adults.
Anismus is usually treated with dietary adjustments, such as dietary fiber supplementation. It can also be treated with a type of biofeedback therapy, during which a sensor probe is inserted into the person's anal canal in order to record the pressures exerted by the pelvic floor muscles. These pressures are visually fed back to the patient via a monitor who can regain the normal coordinated movement of the muscles after a few sessions.
Some researchers have suggested that anismus is an over-diagnosed condition, since the standard investigations or digital rectal examination and anorectal manometry were shown to cause paradoxical sphincter contraction in healthy controls, who did not have constipation or incontinence. Due to the invasive and perhaps uncomfortable nature of these investigations, the pelvic floor musculature is thought to behave differently than under normal circumstances. These researchers went on to conclude that paradoxical pelvic floor contraction is a common finding in healthy people as well as in people with chronic constipation and stool incontinence, and it represents a non-specific finding or laboratory artifact related to untoward conditions during examination, and that true anismus is actually rare.
Etymology and synonyms
Paradoxical anal contraction during attempted defecation in constipated patients was first described in a paper in 1985, when the term anismus was first used. The researchers drew analogies to a condition called vaginismus, which involves paroxysmal (sudden and short lasting) contraction of pubococcygeus (another muscle of the pelvic floor). These researchers felt that this condition was a spastic dysfunction of the anus, analogous to ‘vaginismus’. However, the term anismus implies a psychogenic etiology, which is not true although psychological dysfunction has been described in these patients. Hence:
Latin ani - "of the anus"
Latin spasmus - "spasm"
(Derived by extrapolation with the term vaginismus, which in turn is from the Latin vagina - "sheath" + spasmus - "spasm")
Many terms have been used synonymously to refer to this condition, some inappropriately. The term "anismus" has been criticised as it implies a psychogenic cause. As stated in the Rome II criteria, the term "dyssynergic defecation" is preferred to "pelvic floor dyssynergia" because many patients with dyssynergic defecation do not report sexual or urinary symptoms, meaning that only the defecation mechanism is affected.
Other synonyms include:
Definition
Several definitions have been offered:
Classification
Anismus is classified as a functional defecation disorder. It is also a type of rectal outlet obstruction (a functional outlet obstruction). Where anismus causes constipation, it is an example of functional constipation. Some authors describe an "obstructed defecation syndrome", of which anismus is a cause.
The Rome classification subdivides functional defecation disorders into 3 types, however the symptoms the patient experiences are identical.
It can be seen from the above classification that many of the terms that have been used interchangeably with anismus are inappropriately specific and neglect the concept of impaired propulsion. Similarly, some of the definitions that have been offered are also too restrictive.
Signs and symptoms
Symptoms include:
Cause
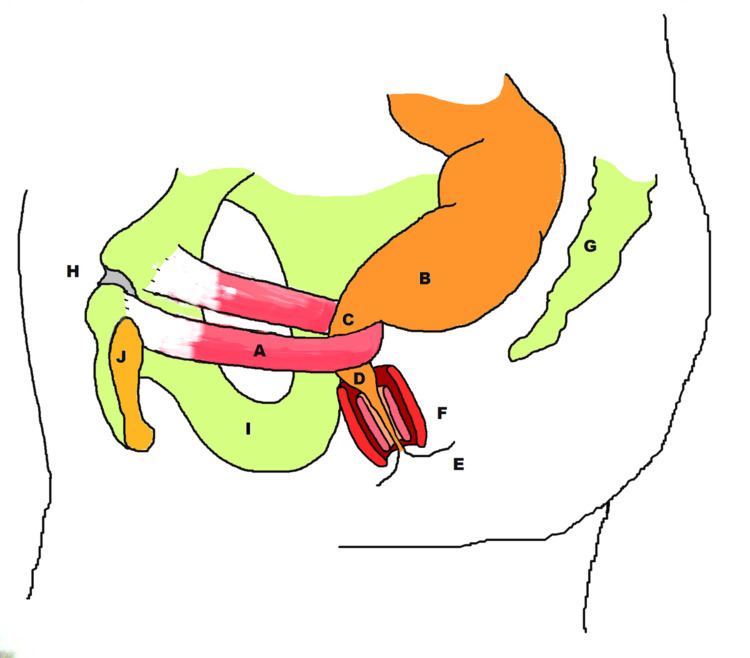
To understand the cause of anismus, an understanding of normal colorectal anatomy and physiology, including the normal defecation mechanism, is helpful. The relevant anatomy includes: the rectum, the anal canal and the muscles of the pelvic floor, especially puborectalis and the external anal sphincter.
The rectum is a section of bowel situated just above the anal canal and distal to the sigmoid colon of the large intestine. It is believed to act as a reservoir to store stool until it fills past a certain volume, at which time the defecation reflexes are stimulated. In healthy individuals, defecation can be temporarily delayed until it is socially acceptable to defecate. In continent individuals, the rectum can expand to a degree to accommodate this function.
The anal canal is the short straight section of bowel between the rectum and the anus. It can be defined functionally as the distance between the anorectal ring and the end of the internal anal sphincter. The internal anal sphincter forms the walls of the anal canal. The internal anal sphincter is not under voluntary control, and in normal persons it is contracted at all times except when there is a need to defecate. This means that the internal anal sphincter contributes more to the resting tone of the anal canal than the external anal sphincter. The internal sphincter is responsible for creating a watertight seal, and therefore provides continence of liquid stool elements.
The puborectalis muscle is one of the pelvic floor muscles. It is skeletal muscle and is therefore under voluntary control. The puborectalis originates on the posterior aspect of the pubic bone, and runs backwards, looping around the bowel.
The point at which the rectum joins the anal canal is known as the anorectal ring, which is at the level that the puborectalis muscle loops around the bowel from in front. This arrangement means that when puborectalis is contracted, it pulls the junction of the rectum and the anal canal forwards, creating an angle in the bowel called the anorectal angle. This angle prevents the movement of stool stored in the rectum moving into the anal canal. It is thought to be responsible for gross continence of solid stool. Some believe the anorectal angle is one of the most important contributors to continence.
Conversely, relaxation of the puborectalis reduces the pull on the junction of the rectum and the anal canal, causing the anorectal angle to straighten out. A squatting posture is also known to straighten the anorectal angle, meaning that less effort is required to defecate when in this position.
Distension of the rectum normally causes the internal anal sphincter to relax (rectoanal inhibitory response, RAIR) and the external anal sphincter initially to contract (rectoanal excitatory reflex, RAER). The relaxation of the internal anal sphincter is an involuntary response. The external anal sphincter, by contrast, is made up of skeletal (or striated muscle) and is therefore under voluntary control. It can contract vigorously for a short time. Contraction of the external sphincter can defer defecation for a time by pushing stool from the anal canal back into the rectum.
Once the voluntary signal to defecate is sent back from the brain, the abdominal muscles contract (straining) causing the intra-abdominal pressure to increase. the pelvic floor is lowered causing the anorectal angle to straighten out from ~90o to <15o and the external anal sphincter relaxes. The rectum now contracts and shortens in peristaltic waves, thus forcing fecal material out of the rectum, through the anal canal and out of the anus. The internal and external anal sphincters along with the puborectalis muscle allow the feces to be passed by pulling the anus up over the exiting feces in shortening and contracting actions.
In patients with anismus, the puborectalis and the external anal sphincter muscles fail to relax, with resultant failure of the anorectal angle to straighten out and facilitate evacuation of feces from the rectum. These muscles may even contract when they should relax (paradoxical contraction), and this not only fails to straighten out the anorectal angle, but causes it to become more acute and offer greater obstruction to evacuation.
As these muscles are under voluntary control, the failure of muscular relaxation or paradoxical contraction that is characteristic of anismus can be thought of as either maladaptive behavior or a loss of voluntary control of these muscles. Others claim that puborectalis can become hypertrophied (enlarged) or fibrosis (replacement of muscle tissue with a more fibrous tissue), which reduces voluntary control over the muscle.
Anismus could be thought of as the patient "forgetting" how to push correctly, i.e. straining against a contracted pelvic floor, instead of increasing abdominal cavity pressures and lowering pelvic cavity pressures. It may be that this scenario develops due to stress. For example, one study reported that anismus was strongly associated with sexual abuse in women. One paper stated that events such as pregnancy, childbirth, gynaecological descent or neurogenic disturbances of the brain-bowel axis could lead to a "functional obstructed defecation syndrome" (including anismus). Anismus may develop in persons with extrapyramidal motor disturbance due to Parkinson's disease. This represents a type of focal dystonia. Anismus may also occur with anorectal malformation, rectocele, rectal prolapse and rectal ulcer.
In many cases however, the underlying pathophysiology in patients presenting with obstructed defecation cannot be determined.
Some authors have commented that the "puborectalis paradox" and "spastic pelvic floor" concepts have no objective data to support their validity. They state that "new evidence showing that defecation is an integrated process of colonic and rectal emptying suggests that anismus may be much more complex than a simple disorder of the pelvic floor muscles."
Complications
Persistent failure to fully evacuate stool may lead to retention of a mass of stool in the rectum (fecal loading), which can become hardened, forming a fecal impaction or even fecoliths.
Liquid stool elements may leak around the retained fecal mass, which may lead to paradoxical diarrhoea and/or fecal leakage (usually known as encopresis in children and fecal leakage in adults).
When anismus occurs in the context of intractable encopresis (as it often does), resolution of anismus may be insufficient to resolve encopresis. For this reason, and because biofeedback training is invasive, expensive, and labor-intensive, biofeedback training is not recommended for treatment of encopresis with anismus.
The walls of the rectum may become stretched, known as megarectum.
Diagnosis
The Rome classification diagnostic criteria for functional defecation disorders is as follows:
The diagnostic criteria for dyssynergic defecation is given as "inappropriate contraction of the pelvic floor or less than 20% relaxation of basal resting sphincter pressure with adequate propulsive forces during attempted defecation."
The diagnostic criteria for inadequate defecatory Propulsion is given as "inadequate propulsive forces with or without inappropriate contraction or less than 20% relaxation of the anal sphincter during attempted defecation."
The Rome criteria recommend that anorectal testing is not usually indicated in patients with symptoms until patients have failed conservative treatment (e.g., increased dietary fiber and liquids; elimination of medications with constipating side effects whenever possible).
Various investigations have been recommended in the diagnosis of anisumus.
Digital rectal examination
Physical examination can rule out anismus (by identifying another cause) but is not sufficient to diagnose anismus.
Anorectal manometry
The measurement of pressures within the rectum and anus with a manometer (pressure-sensing probe).
Evacuation proctography
defecating proctogram, and MRI defecography
Balloon expulsion test
For severe constipation which has not responded to laxatives, dietary supplements or other lifestyle changes. Measures the patients ability to propel a stool through the anal canal. A simulated stool (balloon) is inserted into the rectum with the patient lying on his/her side, and the patient is asked to push the balloon out as they would a stool. Used to assess muscle strength and coordination.
Rectal cooling test
The rectal cooling test is suggested to differentiate between rectal inertia and impaired relaxation/paradoxical contraction
Other techniques include manometry, balloon expulsion test, evacuation proctography (see defecating proctogram), and MRI defecography. Diagnostic criteria are: fulfillment of criteria for functional constipation, manometric and/or EMG and/or radiological evidence (2 out of 3), evidence of adequate expulsion force, and evidence of incomplete evacuation. Recent dynamic imaging studies have shown that in persons diagnosed with anismus the anorectal angle during attempted defecation is abnormal, and this is due to abnormal (paradoxical) movement of the puborectalis muscle.
Treatment
Initial steps to alleviate anismus include dietary adjustments and simple adjustments when attempting to defecate. Supplementation with a bulking agent such as psyllium 3500 mg per day will make stool more bulky, which decreases the effort required to evacuate. Similarly, exercise and adequate hydration may help to optimise stool form. The anorectal angle has been shown to flatten out when in a squatting position, and is thus recommended for patients with functional outlet obstruction like anismus. If the patient is unable to assume a squatting postures due to mobility issues, a low stool can be used to raise the feet when sitting, which effectively achieves a similar position.
Treatments for anismus include biofeedback retraining, botox injections, and surgical resection. Anismus sometimes occurs together with other conditions that limit (see contraindication) the choice of treatments. Thus, thorough evaluation is recommended prior to treatment.
Biofeedback training for treatment of anismus is highly effective and considered the gold standard therapy by many. Others however, reported that biofeedback had a limited therapeutic effect.
Injections of botulin toxin type-A into the puborectalis muscle are very effective in the short term, and somewhat effective in the long term. Injections may be helpful when used together with biofeedback training.
Historically, the standard treatment was surgical resection of the puborectalis muscle, which sometimes resulted in fecal incontinence. Recently, partial resection (partial division) has been reported to be effective in some cases.