
Latin tonsilla pharyngea Dorlands/Elsevier t_13/12812454 FMA 54970 | MeSH A10.549.100 TA A05.3.01.006 | |
 | ||
System Immune system (Lymphatic system) | ||
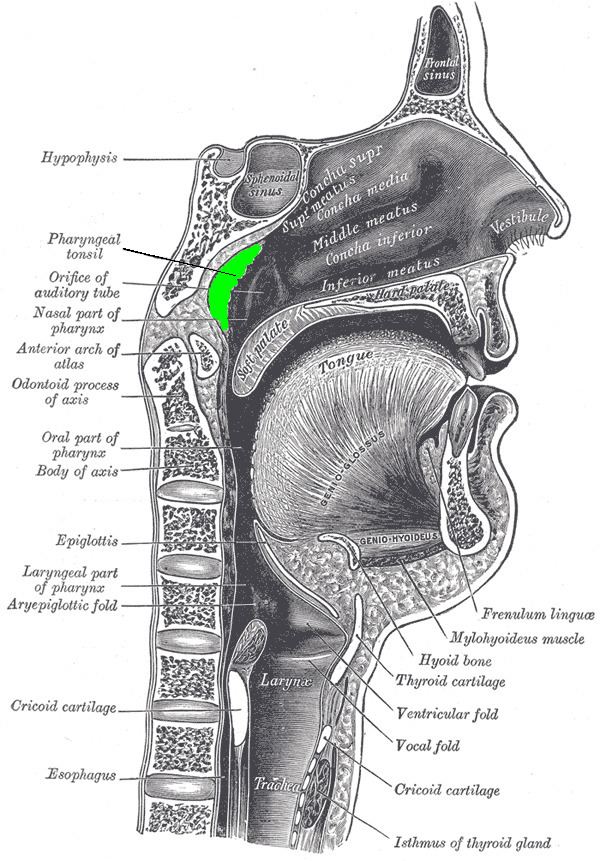
The adenoid, also known as a pharyngeal tonsil or nasopharyngeal tonsil, is the superior-most of the tonsils. It is a mass of lymphatic tissue situated posterior to the nasal cavity, in the roof of the nasopharynx, where the nose blends into the throat. Normally, in children, it forms a soft mound in the roof and posterior wall of the nasopharynx, just above and behind the uvula.
Contents
Structure
The adenoid, unlike the palatine tonsils, has pseudostratified epithelium. The adenoid is often removed along with the palatine tonsils.
Development
Adenoids develop from a subepithelial infiltration of lymphocytes after the 16th week of embryonic life. They are part of the so-called Waldeyer ring of lymphoid tissue which includes the palatine tonsils and the lingual tonsils.
After birth, enlargement begins and continues until aged 5 to 7 years. Symptomatic enlargement between 18 and 24 months of age is not uncommon, meaning that snoring, nasal airway obstruction and obstructed breathing may occur during sleep. However, this may be reasonably expected to decline when children reach school age, and progressive shrinkage may be expected thereafter.
The establishment of the upper respiratory tract is initiated at birth. Species of bacteria such as lactobacilli, anaerobic streptococci, actinomycosis, Fusobacterium species, and Nocardia are normally present by 6 months of age. Normal flora found in the adenoid consists of alpha-hemolytic streptococci and enterococci, Corynebacterium species, coagulase-negative staphylococci, Neisseria species, Haemophilus species, Micrococcus species, and Stomatococcus species.
Clinical significance
An enlarged adenoid, or adenoid hypertrophy, can become nearly the size of a ping pong ball and completely block airflow through the nasal passages. Even if the enlarged adenoid is not substantial enough to physically block the back of the nose, it can obstruct airflow enough so that breathing through the nose requires an uncomfortable amount of work, and inhalation occurs instead through an open mouth. The enlarged adenoid can also obstruct the nasal airway enough to affect the voice without actually stopping nasal airflow altogether.
Adenoid facies
Enlargement of the adenoid, especially in children, causes an atypical appearance of the face, often referred to as adenoid facies. Features of adenoid facies include mouth breathing, an elongated face, prominent incisors, hypoplastic maxilla, short upper lip, elevated nostrils, and a high arched palate. George Catlin, in his book Breath of Life, published in 1861, illustrates adenoid facies in many engravings, and advocates nose-breathing.
Removal
Surgical removal of the adenoid is a procedure called adenoidectomy. Adenoid infection may cause symptoms such as excessive mucus production, which can be treated by its removal. Studies have shown that adenoid regrowth occurs in as many as 19% of the cases after removal. Carried out through the mouth under a general anaesthetic (or less commonly a topical), adenoidectomy involves the adenoid being curetted, cauterized, lasered, or otherwise ablated.